 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 10 Issue 1 - April 2019
Clinico-etiological profile of children with thrombocytosis at SRTRH GMC, Ambojogai
Sambhaji Chate1, Sunil Holikar2, Shubhangi Indorkar3*
1Professor, 2Associate Professor, 3Junior Resident, Department of Pediatrics, Swami Ramanand Teerth Rural Government Medical College, Ambajogai, Beed-431517, Maharashtra, INDIA. Email: shubh25989@gmail.com
Abstract Background: Thrombocytosis (TS) or elevation in the peripheral blood platelet count to values >400,000/µL is common in infancy and childhood, occurring in 3 to 13% of children Aims and Objectives: To Study of Thrombocytosis in pediatric age group. Methodology: This was cross-sectional study carried out in the department of pediatrics at tertiary health care centre in the patients who showed thrombocytosis on CBC during the One year period were studied. During the one year there were 102 patients who showed thrombocytosis. The causative factor in each patient was identified. The data was entered in excel sheet and analyzed by excel software for windows 10. Result: The majority of the patients were in the age groups 6m-2yr were 53.92% followed by 1m-6m; Were 18.62%, 2yr-6yr were 14.70% 6yr-12yr were 12.74%. The majority of the patients were Male were 57.84% and Female were 42.15%. The Majority of the patients with Severe thromocytosis were in the age groups 6Y-12Y were - 15.38%, Moderate were common in 2Y-6Y - 13.33% and 1M-6M were 10.53%; Mild were more common in 6M-2Y -92.73% followed by 2Y-6Y - 86.67%. All the patients were of Secondary thrombocytosis, no patient of primary thrombocytosis found.The most common causes were Infection- i.e. Respiratory tract infection in 48% followed by Gastrointestinal tract infection in 18.60%, Central nervous system infection in 4.90%, Urinary tract infection in 2.94%, Skin infection in 0.98%, Connective tissue infection in 0.98%; Nutritional causes were Iron deficiency anemia-4.90%, SAM-1.96%, SAM with megaloblastic anemia in 0.98%; Hymolytic anemia in the B Thalassemia was 3.92%, Diamond blackfan syndrome was 0.98%, In Inflammation – Arthritis was 0.98%; In Tumors- Post auricular rhabdomyosarcoma was 0.98%, Postsplenectomy was 0.98%, In Allergic, Urticaria was 1.96%, Miscellaneous were 1.96%; Soap ingestion was 0.98%; Post MR vaccination was 0.98%; Fever(unspecified) was 3.92% Conclusion: It can be concluded from our study that majority of the patients were were in the age groups 6m-2yr, The majority of the patients were Male, The Majority of the patients with Severe thromocytosis were in the age groups 6Y-12Y, Moderate were common in 2Y-6Y , Mild were more common in 6M-2Y, The most common causes were Infection- i.e. Respiratory tract infection in 48% followed by Gastrointestinal tract infection , Nutritional causes were Iron deficiency anemia. Key Word: Thrombocytosis(TS), IDA (Iron deficiency Anemia), SAM (Severe Acute Malnutrition, LRTI (Lower Respiratory Tract Infection).
INTRODUCTION Thrombocytosis (TS) or elevation in the peripheral blood platelet count to values >400,000/µL is common in infancy and childhood, occurring in 3 to 13% of children1. Extreme thrombocytosis (platelets >1,000,000/µL) is uncommon, occurring in less than 2% of children2, but may be more common in critically ill children3. Thrombocytosis is classified according to its origin into primary and secondary forms. Primary (clonal) thrombocytosis is a myeloproliferative disorder, caused by abnormal and uncontrolled expansion of haematopoietic cells, which is likely to be complicated by thromboembolism4. Secondary (or reactive) thrombocytosis is due to a variety of underlying conditions like infection, inflammation, iron deficiency, tissue damage, hemolysis, severe exercise, malignancy, hyposplenism, and other causes of an acute phase response5. In older adults an elevated platelet count can signify an underlying hematological disease, in children in almost every case the elevated platelet count is due to another medical condition, such as acute infection, chronic inflammation, collagen vascular and renal diseases, Langerhan’s cell histiocytosis, iron deficiency, hemolytic anemia, and Kawasaki disease (KD)6-7. Drugs are another less frequent cause of secondary thrombocytosis in children8-9 So we have studied Thrombocytosis in pediatric age group with respect to various etiology in the pediatric age group.
METHODOLOGY This was cross-sectional study carried out in the department of pediatrics at tertiary health care centre in the patients who showed thrombocytosis on CBC during the One year period were studied. During the one year there were 102 patients who showed thrombocytosis. After written and explained consent all details of the patients like age, sex, clinical features, undergone routine investigations like CBC, X-ray, other necessary investigations if needed was carried out. The causative factor in each patient was identified. The data was entered in excel sheet and analyzed by excel software for windows 10. RESULT Table 1: Distribution of the patients as per the age
The majority of the patients were in the age groups 6m-2yr were 53.92% followed by 1m-6m Were 18.62%, 2yr-6yr were 14.70% 6yr-12yr were 12.74%.
Table 2: Distribution of the patients as per sex
The majority of the patients were Male were 57.84% and Female were 42.15%
Table 3: Distribution of the patients as per severity of thrombocytosis and age group
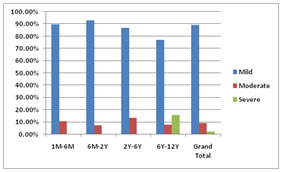
The Majority of the patients with Severe thromocytosis were in the age groups 6Y-12Y were - 15.38%, Moderate were common in 2Y-6Y - 13.33% and 1M-6M were 10.53%; Mild were more common in 6M-2Y -92.73% followed by 2Y-6Y - 86.67%. Graph 1: Distribution of the patients as per severity of thrombocytosis and age group
Table 4: Distribution as per the type of thrombocytosis
All the patients were of Secondary thrombocytosis, no patient of primary thrombocytosis found.
Table 5: Distribution as per the etiology of thrombocytosis
The most common causes were Infection- i.e. Respiratory tract infection in 48% followed by Gastrointestinal tract infection in 18.60%, Central nervous system infection in 4.90%, Urinary tract infection in 2.94%, Skin infection in 0.98%, Connective tissue infection in 0.98%; Nutritional causes were Iron deficiency anemia - 4.90%, SAM-1.96%, SAM with megaloblastic anemia in 0.98%; Hymolytic anemia in the B Thalassemia was 3.92%, Diamond blackfan syndrome was 0.98%, In Innflammation– Arthritis was 0.98%; In Tumors- Postauricular rhabdomyosarcoma was 0.98%, Postsplenectomy was 0.98%, In Allergic , Urticaria was 1.96%, Miscellaneous were 1.96%; Soap ingestion was 0.98%; Post MR vaccination was 0.98%; Fever(unspecified) was 3.92%
DISCUSSION Thrombopoietin (Tpo) is the key regulator of platelet production in humans, and is primarily expressed in the liver, and to a lesser extend the kidneys, bone marrow and other organs. It acts on the commitment of hematopoietic stem and progenitor cells into platelet-specific differentiation through its c-mpl receptor that is also expressed on pluripotent megakaryocytes, platelets, and endothelial cells. C-mpl receptors normally remove circulating Tpo by cellular absorption and internalization. Hepatic Tpo expression is unchanged in the presence of thrombocytopenia. Tpo serum concentrations are normal if thrombocytopenia results from platelet destruction, while are elevated if thrombopoiesis drops. Longitudinal Tpo measurements in infants and children with acute infections, surgical trauma and other conditions show that the elevation of circulating Tpo concentration precedes TS10,11,12) Tpo serum levels are significantly higher in patients with ET than in patients with reactive TS, although Tpo serum levels are not correlated with platelet counts in patients with ET(50). Besides Tpo, other cytokines or hematopoietic growth factors, such as stem cell factor, granulocytemacrophage colony stimulating factor, IL-6, IL-8 and IL-11 play a major role in certain steps of megakaryopoiesis and thrombopoiesis(13,14,15).Secondary or reactive thrombocytosis in childhood results from increased thrombopoiesis, as a reactive process due to an underlying infection, chronic inflammation, injury, malignancy, and surgical or functional splenectomy16.In our study we have seen The majority of the patients were in the age groups 6m-2yr were 53.92% followed by 1m-6m; Were 18.62%, 2yr-6yr were 14.70% 6yr-12yr were 12.74%. The majority of the patients were Male were 57.84% and Female were 42.15%. The Majority of the patients with Severe thromocytosis were in the age groups 6Y-12Y were - 15.38%, Moderate were common in 2Y-6Y - 13.33% and 1M-6M were 10.53%; Mild were more common in 6M-2Y -92.73% followed by 2Y-6Y-86.67%. All the patients were of Secondary thrombocytosis, no patient of primary thrombocytosis found. The most common causes were Infection- i.e. Respiratory tract infection in 48% followed by Gastrointestinal tract infection in 18.60%, Central nervous system infection in 4.90%, Urinary tract infection in 2.94%, Skin infection in 0.98%, Connective tissue infection in 0.98%; Nutritional causes were Iron deficiency anemia -4.90%, SAM-1.96%, SAM with megaloblastic anemia in 0.98%; Hymolytic anemia in the B Thalassemia was 3.92%, Diamond blackfan syndrome was 0.98%, In Inflammation–Arthritis was 0.98%; In Tumors- Post auricular rhabdomyosarcoma was 0.98%, Postsplenectomy was 0.98%, In Allergic , Urticaria was 1.96%, Miscellaneous were 1.96%; Soap ingestion was 0.98%; Post MR vaccination was 0.98%; Fever(unspecified) was 3.92% These findings are similar to Sarangi R et al17 they found Out of 2500 hemograms done in pediatrics age group, 272 (10.8%) patients showed thrombocytosis. About 99.6% of cases were of secondary thrombocytosis. Only one case of primary thrombocytosis was encountered. The most common cause of secondary thrombocytosis was infection (39.5%) alone followed by iron deficiency anemia (14.1%).
CONCLUSION It can be concluded from our study that majority of the patients were were in the age groups 6m-2yr, The majority of the patients were Male, The Majority of the patients with Severe thromocytosis were in the age groups 6Y-12Y, Moderate were common in 2Y-6Y, Mild were more common in 6M-2Y, The most common causes were Infection- i.e. Respiratory tract infection in 48% followed by Gastrointestinal tract infection , Nutritional causes were Iron deficiency anemia.
REFERENCES
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.