 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 10 Issue 1 - April 2019
Association of serum 25-hydroxy vitamin d levels and recurrent wheezing in children under five years of age: A case control study
Neerupam Gupta1*, Naine Bhadrala2, Anuj Kapoor3
1Department of Pediatrics, Government Hospital Sarwal, Directorate of Health Services, Jammu, J and K, INDIA. 2Department of Anesthesiology, Government Medical College Jammu, J and K INDIA. 3Sr. Resident Government Medical College Kathua, J and K, INDIA. Email: neroped@gmail.com
Abstract Background: Vitamin D deficiency has been declared a public health problem for children worldwide. Serum 25-hydroxy vitamin D is found to be associated with wide range of pulmonary diseases including wheezing in children. Methods: A hospital based case control study was conducted in subdistrict hospital Sarwal Jammu from Feb 2017 to Jan 2019. A total of 86 children under the age of five years attending pediatric OPD for cough with wheezing were enrolled as cases. Equal number of children with similar profile attending immunization centre were enrolled as controls. An informed consent was obtained from all participants. Trained phlebotomist collected venous blood sample for vitamin D levels. Vitamin D deficiency was characterized as per IAP criteria. Results were presented in the form of percentages and odds ratio was calculated as measure of associates. Results: Out of 86 patients with wheezing ,18 (20.9 %) had deficient vitamin D levels and 38 (44.1%) had insufficient vitamin D levels as compared to control group where deficient vitamin D levels were found in 9 (10.4%) patients and insufficient levels were found in 29 (33.72%) children. Conclusions: Study findings revealed a high prevalence of vitamin D deficiency in children with recurrent wheezing. Prompt management of vitamin D deficiency should be considered among children with wheezing. Key Word: case control study, 25 hydroxy vitamin D, wheezing.
INTRODUCTION Vitamin D is a fat soluble nutrient which is a modulator of calcium absorption and bone health. It also plays an important role in immune regulation and in respiratory infections 1,2. Serum 25OHD is the best indicator of vitamin D status in body. Vitamin D deficiency has a high incidence worldwide. It is estimated that almost half of the healthy people are 25 OHD deficient3. Insufficient sun exposure or pigmented skin and inadequate dietary intake are the main causes of these low levels of vitamin D. There has been growing recognition of the extra skeletal role of vitamin D in recent years. Vitamin D plays a significant role in inborn and adaptive immunity4,5. It was documented that the global rise of asthma and allergic diseases may be linked to lower vitamin D6,7. The greatest burden of allergic diseases are during childhood at which time the rapidly rising rates of diseases are most evident in population. Recurrent wheezing in young children either transient or that will continue as asthma, can be severe and cause significant impairment in quality of life with frequent visits to health professionals8,9. It is estimated that about one third of school age children manifest the wheezing during the first 5 years of life8. The most common causes of wheezing in preschool children are bronchiolitis and asthma. The aim of the present study was to assess the possible role of vitamin D status on occurrence of wheezing in children under five years of age.
METHODS This was a hospital based case control study done in department of paediatrics Govt Hospital Sarwal for a period of 12 months after obtaining approval from ethics committee of the institution. A total of 86 cases and controls were enrolled in study. Children under the age of five years diagnosed with wheeze presenting to emergency/out patient department were enrolled after getting informed written consent. Wheezing was confirmed by the clinical examination. Recurrent wheeze was defined as three or more episodes of parentally reported wheeze in past 12 months of life. Healthy age and weight matched children visiting for immunization were taken as controls. Detailed history of wheezing episodes along with therapy, dietary history, sunlight exposure, respiratory system examination and anthropometry were recorded. Those with underlying chronic illness, malnutrition, clinical rickets, congenital heart disease, congenital malformations predisposing to respiratory distress and having received therapeutic dose of vitamin D (3 lakh - 6 lakh units) in last six months were excluded. 2 ml blood sample was taken from the peripheral vein of each participant by a trained phlebotomist. The sample was immediately transferred to a accredited laboratory for testing. In order to categorize various degrees of vitamin D deficiency authors used criteria that was mentioned in Indian academy of paediatrics 2017 guidelines on vitamin D deficiency. Based on these criteria sufficient are defined as levels more than 20 ng/ml , insufficient as 12 – 20 ng/ml and deficient as levels less than 12 ng/ml. Data was recorded on a pre-designed proforma and managed on Excel spread sheet. All the entries were double checked for any possible key-board error. Statistical significance between two variables was determined using Student’s t-test. Chi-square was performed to test for differences in proportions of categorical variables between two groups. Odds ratio (OR) was calculated with 95 % confidence interval. A p value of less than 0.05 was considered statistically significant.
RESULTS A total of 86 under five children with recurrent wheeze were enrolled as cases and similar number of healthy children attending immunization clinic were enrolled as controls. The demographic characteristics were comparable in both the groups (Table 1). Table 1: Age and Gender distribution of cases and controls
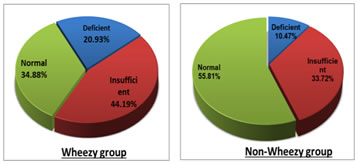
Among cases 18 patients had (20.94%) deficient vitamin D levels as compared to controls where only 9 (10.47%) children were deficient and this difference is statistically significant (p value 0.01). Similarly among cases 38 (44.18%) subjects had insufficient vitamin D levels as compared to controls where only 29 (33.72%) children had insufficient levels and also this difference is statistically significant (p value 0.029). (Table 2) and (Figure 1) Table 2: Distribution of cases and controls according to Vitamin D status
Figure 1: Percentage Distribution of Vitamin D status in cases and controls Significant association of vitamin D levels was seen with occurrence of recurrent wheezing in under five children (p value < 0.05). Children with deficient vitamin D levels were at 3 times (OR 3.2) higher risk of having recurrent wheezing as compared to kids with normal vitamin D levels whereas children with insufficient vitamin D levels were at 2 times (OR 2.09) higher risk of having recurrent wheezing as compared to kids with normal vitamin D levels. (Table 3) Table 3: Association of vitamin D levels with recurrent wheezing
p- value > 0 .05 statistically significant; p- value > 0.01 statistically highly significant
DISCUSSION Vitamin D deficiency is a global health problem. It has been reported that the prevalence of vitamin D deficiency ranges from 69% - 82% in Indian population (10). The high frequency of vitamin D deficiency in our country may be related to inadequate vitamin D supplementation during infancy, low levels of vitamin D during pregnancy and scarcity of vitamin D fortified food products11. Studies conducted in Finland and Japan on more than 750 mother child pair have found that dietary vitamin D intake is inversely related to the incidence of wheezing in children12. Sunlight exposure is an important factor in vitamin D synthesis. The limited exposure seems to be due to change in life style. Studies have shown that a minimum 30 minute weekly sunlight exposure in bright sunlight over 40 % body area for at least four months is required to achieve sufficient vitamin D by 6 months of age in breast fed infants13,14. Wheezing during early life represents a common disorder characterized by airway obstruction. About one in every three children have at least one episode of wheezing prior to their third birthday and cumulative prevalence of wheeze is around 50 % at six years of age15,16,17. The present study was aimed at finding an association between vitamin D levels and recurrent wheeze in children below five years of age. We found that 20.94 % of children in wheezy group were vitamin D deficient as compared to control group where 10.47 % children were deficient. Similarly insufficient vitamin D levels were found in 44.18 % of wheezy children as compared to 33.72 % of controls. Both the differences are statistically significant. Several epidemiological studies suggest that low levels of vitamin D during early life is inversely associated with the risk of developing respiratory infections and wheezing in childhood. Our study revealed a three times higher risk of developing wheeze in vitamin deficient and two times higher risk in vitamin D insufficient children under five years. Similar results were found by Prasad et al who reported that each 10ng /ml decrease in vitamin D levels is associated with 7.25% greater odds of wheezing in childhood18. Kumar et al reported that serum vitamin D level below 17.5 ng/ml predisposes for recurrent wheezing episodes and decrease in its level by 1ng/ml in serum increases the chances of wheezing by 7.3%19. In 2014 Stenberg Hammer et al demonstrated that subnormal levels of vitamin D are associated with acute wheeze in preschool children20. Bener et al compared vitamin D status of allergic and healthy children and found the frequency of severe vitamin D deficiency was significantly higher in children with wheezing (23%) than in healthy children (10.5%)21. Similar results were found in other studies22,23,24. Vitamin D has an important role in the lung development and regulation of innate and adaptive immunity. Vitamin D derangement posting as a possible risk for wheezing could be attributed to its potential role in the pathogenesis of atopy25 or involvement in lung development26 and not only to the reported increased incidence of respiratory viral infections27. Vitamin D directly and indirectly induces production of antimicrobial proteins and has other antimicrobial effects28,29. Moreover evidence suggests that vitamin D deficiency in early life may lead to permanent susceptibility to respiratory problems and poorer respiratory outcomes that are not atopy related26. So we conclude that there is enough evidence that vitamin D plays an important role in respiratory diseases like asthma and wheeze in children. So vitamin D supplementation should be considered in under five children presenting with recurrent wheezing.
REFERENCES
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.