 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 10 Issue 1 - April 2019
Effectiveness of non-invasive hand held transcutaneous bilirubinometer for the diagnosis of neonates with hyperbilirubinemia
Prakhar Mohniya1*, Prashant Shah2, C D Aundhakar3, Amit Galgali4
1Senior Resident, SNMC, Agra, Uttar Pradesh, INDIA. 2Assistant Professor, 3Professor, Department of Pediatrics, Krishna Institute of Medical Science, Karad, Maharashtra, INDIA. 4Junior Consultant Health Care Global, Bangalore, Karnataka, INDIA.
Abstract Background: Clinical evaluation of neonatal jaundice based on visual assessment on the depth of jaundice is subjective and inaccurate which can be confounded by skin colour and haemoglobin. Various methods have been developed to aid non-invasive diagnosis of hyperbiliruneamia and total serum bilirubin. Transcutaneous bilirubinometer is hand held, non- invasive method. Aim: To assess the effectiveness of non-invasive hand held transcutaneous bilirubinometer for the diagnosis of neonates with hyperbilirubinemia. Material and Methods: Two hundred randomly selected eligible full term normal neonates delivered in hospital were included in the study. Bilirubin was estimated within 24 hours by laboratory investigation, again blood sample was collected in sterile container on day 3, day 5 and day 7 and serum bilirubin of particular day was also recorded by transcutaneous bilirubinometer for the comparison with its lab value. Results: Transcutaneous bilirubin over forehead as well as over sternum showed a good correlation with total cord bilirubin; the highest correlation coefficient was significant in both cases (P<0.05). Conclusion: TCB method can be used for diagnosis of hyperbilirubinemia with very high sensitivity rate. TCB over sternum give slightly better yield then TCB over forehead as far as the sensitivity and specificity is concerned. Key Word: Neonates, hyperbilirubinemia, Transcutaneous bilirubinometer, sensitivity, specificity
INTRODUCTION Neonatal hyperbilirubinemia is a term for elevated total serum bilirubin in newborns and infants less than one month of age. The immediate goal of screening for elevated bilirubin levels is to assess risk for hyperbilirubinemia requiring treatment.1 Often a pediatrician is interested to corroborate his clinical estimate of the icterus with actual serum bilirubin level. Any such technique should ideally be accurate, non-invasive and valid. A large number of studies have tested the agreement between transcutaneous bilirubinometer results and TSB.2-5 Most studies have found fair to excellent correlation between the two. However, the ‘correlation’ is not an appropriate statistical technique for judging the agreement. Earlier instruments have been found more useful in whites and some other population; studies in India have not reported the same degree of agreement. While the correlation may be good, the difference between two values may be too large to be acceptable clinically. Despite limitations, transcutaneous bilirubinometers can serve as a screening tool, especially where services of a neonatologist are not available. This can be very helpful in the community or peripheral health setup for the grass root level workers to screen neonatal hyperbilirubinemia. Therefore, the present study was conducted to assess the effectiveness of non-invasive hand held transcutaneous bilirubinometer for the diagnosis of neonates with hyperbilirubinemia. MATERIAL AND METHODS This cross sectional study was conducted on full term normal neonates delivered in hospital over a period of two years. Two hundred randomly selected eligible full term normal neonates delivered in hospital were included in the study. Patients were included in the study after taking the voluntary informed consent of their parents. The random selection of the cases who met the inclusion criteria were done by tossing a coin. If the head comes, then that participant was included in the study. Both the genders were included in the study. Inclusion criteria
Exclusion criteria
Ethical issues: First of all, the study protocol was approved by the Scientific and Ethical Committee of the Institution. All the participant’s parents were also informed about the study procedure and the information required from them for the study. A voluntary informed written consent was taken from the participant’s parents those who consented were included in the study. A strict confidentiality was maintained about the personal details of the participants and information related to the study. The questionnaire included the information regarding mother’s age, parity, gestational hypertension, gestational diabetes, mode of delivery, birth weight, APGAR score and birth weight. Umbilical cord mixed blood samples was collected in a sterile container drawn from placental side of the umbilical cord incised while severing it at the time of birth of the baby. The mother’s age, parity, residence, community, blood pressure, diabetes, use of iodine antiseptics on the mother prior to delivery will be recorded. The type of medications/anesthesia given including doses used, duration of anesthesia given to the mother till birth of the baby were recorded. At birth, the babies weight, sex, time to first cry, congenital abnormalities, Apgar scores was noted. Bilirubin was estimated within 24 hours by laboratory investigation, again blood sample was collected in sterile container on day 3, day 5 and day 7 by all aseptic means and serum bilirubin of particular day was also recorded by transcutaneous bilirubinometer for the comparison with its lab value. Statistical Analysis: Data management and analysis was done using Microsoft excel and Epi-info software. The categorical variables were assessed using Pearson Chi-square. Sensitivity, specificity, positive predictive value, negative predictive value were assessed and the study subjects were compared using suitable statistical tests.
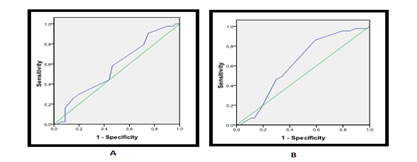
RESULTS To assess the effectiveness of non-invasive hand held Trans-cutaneous bilirubinometer from Drager JM-103, a cross sectional study was conducted among 200 normal neonates. Out of 200 neonates, 90 (45%) were female child while 110 (55%) were male child, with female to male sex ratio of 0.81:1. Before the completion of the study 18 (9%) neonates lost to follow up. They were not turned up for follow up visit. Total 137 (68.5%) children were discharged to home while 45 neonates were found with hyperbilirubinemia during study period and were admitted in the NICU for phototherapy. Transcutaneous Bilirubin level over forehead and sternum taken at different interval were compared with total serum Bilirubin level taken at the same time. On the first day, bilirubin value by TCB over forehead and sternum both methods were positively correlated with cord blood Bilirubin value with r2 value over 0.8 indicating strong linear correlation. On the third day Bilirubin value by both TCB methods were positively correlated with conventional serum Bilirubin value with r2 value more than 0.95 indicating strong linear correlation. On the fifth day Bilirubin value by both TCB methods were positively correlated with conventional serum Bilirubin value with r2 value 0.95 indicating strong linear correlation. On the seventh day Bilirubin value by both TCB methods were positively correlated with conventional serum Bilirubin value with r2 value 0.9 indicating strong linear correlation. The efficacy of Trans cutaneous Bilirubin level was measure to diagnose hyperbilirubinemia in normal neonate. The following two graphs shows ROC curve of the TCB level at day 1 immediately after birth: Figure 1: ROC curve for Bilirubin by TCB over a. forehead b. sternum
The present study investigated the transcutaneous Bilirubin over sternum and forehead and the total cord bilirubin measurement by a direct spectrophotometric method in the laboratory. Transcutaneous bilirubin over forehead as well as over sternum both showed a good correlation with total cord bilirubin; the highest correlation coefficient was significant in both cases (P<0.05). Transcutaneous bilirubin cut off values of 2.4 mg/dl and 2.6 mg/dl, for TCB over forehead and sternum respectively, have highest sensitivity and specificity. Both the TCB value over sternum and forehead were very well correlated, however TCB over sternum give slightly better yield then TCB over forehead as far as the sensitivity and specificity is concerned. Bilirubin value of 5.1mg/dl by TCB over forehead indicates hyperbilirubinemia with sensitivity of 90.7%. Bilirubin value of 4.75 mg/dl by TCB over sternum indicates hyperbilirubinemia with sensitivity of 93%. Thus, TCB method can be used for diagnosis of hyperbilirubinemia with very high sensitivity rate. TCB over sternum give slightly better yield then TCB over forehead as far as the sensitivity and specificity is concerned.
DISCUSSION Jaundice is a clinical condition that is present in pediatric practice and constitutes one of the major issues within the neonatal period. It occurs in both physiological and pathological processes in newborns.1 In the present study, the mean level of bilirubin was 1.75 mg/dl with standard deviation of 0.54. Cord blood bilirubin level was divided in to ‘less than 1.78 or mg/dl’ and ‘1.78 mg/dl or more’. There were 113 (56.5%) cases having S. bilirubin less than 1.78 mg/dl while remaining had level 1.78 or more. At day three based on the serum Bilirubin level 43 (21.5%) neonate had hyperbilirubinemia while in remaining 157 (78.5%) cases bilirubin level within normal limit. These results are comparable with the studies in which it is also mentioned that neonatal jaundice usually appears 2-4 days after birth.6 The present study investigated the transcutaneous Bilirubin over sternum and forehead and the total cord bilirubin measurement by a direct spectrophotometric method in the laboratory. In our study, transcutaneous bilirubin over forehead as well as over sternum both showed a good correlation with total cord bilirubin; the highest correlation coefficient was significant in both cases (P<0.05). Transcutaneous bilirubin cut off values of 2.4 mg/dl and 2.6 mg/dl, for TCB over forehead and sternum respectively, have highest sensitivity and specificity. A study by Tommy SK et al investigated the trancutaneousblirubin using the paired transcutaneous bilirubin measurements by the JM-103 Minolta and the total serum bilirubin measurement by a direct spectrophotometric method in the laboratory. The mean age of the 113 neonates at the time of data collection was five days (range = 3-7 days and >30 weeks of gestational age). Transcutaneous bilirubin showed a good correlation with total serum bilirubin; the highest correlation coefficient was 0.83 (P<0.001). Transcutaneous bilirubin cutoff values of 230 μmol/L and 298 μmol/L could have 100% sensitivity and specificity respectively, to predict a total serum bilirubin level of higher than 250 μmol/L (the accepted threshold for treatment). However, when the mean difference between transcutaneous and total serum bilirubin was 14 μmol/L (standard deviation, 28 μmol/L; P<0.001); the JM-103 tended to overestimate total serum bilirubin. The 95% limits of agreement were between 40 and 69 μmol/L. The author concluded that the JM-103 can be used safely in the Emergency Departments (AED) or Maternal and Child Health Centres (MCHC) for healthy-looking neonates aged 3 to 7 days; a transutaneous bilirubin (maxTcB) of less than 230 μmol/L can be used to let the patient return home for follow-up.7In another study, a new transcutaneous bilirubinometer (JM-103 Minolta Airshields) for detection of hyperbilirubinaemia in term or near-term healthy Chinese newborn was evaluated. TcB was significantly correlated with TSB, with a correlation coefficient of 0.83 (p= 0.001). Their mean difference was 21.7 mmol/l (SD 21.2, p=0.001), with the 95% limits of agreement between 219.9 and 263.3 mmol/ l. In both low-risk and medium-risk thresholds for phototherapy, using the 75th centile of Bhutani’s nomogram as threshold, TcB could identify all cases. It had a sensitivity and negative predictive value of 100% each, a specificity of 56% and positive predictive value of 23% for high-risk cases, using the 75th percentile as cut-off, the sensitivity and negative predictive value were reduced to 86.7% and 97.0%, respectively. An accurate point-of-care bilirubin analyser facilitates bilirubin screening and avoids unnecessary blood tests.8A study by Suwinol et al had compared the accuracy of two transcutaneous bilirubinometer JM103 (JM) and SpectRx, Bilicheck (BC) in estimating total serum bilirubin (TSB) level. The correlation coefficients between TcB (JM and BC) and TSB measurements were significant and similar (r 0.80 and 0.82, respectively). The sensitivity of BC was higher, but specificity was lower, than JM in corresponding to different TSB levels, except at a TSB level of 15 mg/dl (256.5µmol/L) when both instruments yielded 100% sensitivity. The accuracy of JM in predicting TSB was higher than BC at all TSB levels. Operating the JM was simple and uncomplicated. It would be suitable for clinical use when a number of personnel perform the measurement. Comparison between transcutaneous bilirubin measured by JM and BC had similar correlation to TSB. Accuracy in predicting TSB at specific levels for JM was higher than BC.9A study by Maisels MJet al evaluated the JM-103 in 849 newborns more than 35 weeks of gestation in 3 hospitals. These infants had total serum bilirubin (TSB) levels measured on clinical indication, and transcutaneous bilirubin (TcB) levels were obtained within one hour of the Total Serum Bilirubin (TSB) levels. The population was 59.2% white, 29.8% black, 4.5% East Asian, 3.8% Middle Eastern, 1.6% Indian/Pakistani, and 1.1% Hispanic. There was a close correlation between TSB and TcB values in all of the population groups: white (n=503, r=0.949); black (n =253, r=0.822); and East Asian, Indian/Pakistani, and Hispanic (n=93, r=0.926). In the black population, the correlation was less close than in the other groups, and differences between the TcB and TSB measurements tended to increase with rising TSB values. JM-103 values differed from TSB values by 3 mg/dL or more in 2% of white, 3.2% of other, and 17.4% of black infants. In these black infants, the JM-103 value was always greater than the TSB value. The correlation in black infants was not as close as in other groups, but there was a tendency in blacks was for the JM-103 to overestimate serum bilirubin levels. However, the author revealed that the measurement technique was rapid and simple, and it was easy to perform repeated measurements over time, thus reducing the likelihood of error. Serum bilirubin measurements are still required when treatment with phototherapy or exchange transfusion is being considered.10In present study, Both the TCB value over sternum and forehead were very well correlated, however TCB over sternum give slightly better yield then TCB over forehead as far as the sensitivity and specificity is concerned. Bilirubin value of 5.1mg/dl by TCB over forehead indicates hyperbilirubinemia with sensitivity of 90.7%. Bilirubin value of 4.75 mg/dl by TCB over sternum indicates hyperbilirubinemia with sensitivity of 93%. Thus, TCB method can be used for diagnosis of hyperbilirubinemia with very high sensitivity rate. TCB over sternum give slightly better yield then TCB over forehead as far as the sensitivity and specificity is concerned. REFERENCES
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.