 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 10 Issue 1 - April 2019
Neerupam Gupta1*, Naine Bhadrala2, Harman Multani3
1Department of Pediatrics, Government Hospital Sarwal, Directorate of Health services, Jammu, J and K, INDIA. 2Department of Anesthesiology, Government Medical College Jammu, J and K, INDIA. 3Department of Microbiology, Sr. Resident Govt. Medical College Jammu, J and K, INDIA. Email: neroped@gmail.com
Abstract Background: To compare the effects of general anaesthesia and spinal anaesthesia on Apgar score in full term neonates born to elective caesarean section. Methods: The study was conducted on 90 healthy full term patients of ASA 1 and 2 category presenting for elective lower segment caesarean section (LSCS). 45 patients were given general anaesthesia and other 45 received spinal anaesthesia. The Apgar score was recorded at 1 minute and 5 minutes after birth. Results: Out of 45 mothers who received general anaesthesia, 38 (84.4%) gave birth to neonates having Apgar score less than or equal to 6 at 1 minute after birth and the remaining 7 neonates (15.6%) had Apgar score of more than 7. Out of 38 babies only one baby continued to have Apgar score of less than or equal to 6 at 5 minutes. On the other hand, out of 45 mothers who received spinal anaesthesia, only 15 mothers gave birth to babies having Apgar score less than or equal to 6 at 1 minute after birth out of which 14 improved at 5 minutes with Apgar score of more than or equal to 7. Conclusion: We conclude based on the study results that babies born by LSCS under general anaesthesia are at higher risk of having low Apgar score (Less than or equal to 6) at 1 minute after birth. Key Word: Caesarean Section, General Anaesthesia, Spinal Anaesthesia, Apgar score
INTRODUCTION The choice of anaesthesia for obstetric cases has been traditionally influenced by patient and physician preferences. It can be performed under general or regional anaesthesia like spinal or epidural technique. The obstetric anaesthetist requires special training and skills to provide safe anaesthesia. The anaesthetic techniques and agents chosen should provide good anaesthesia and analgesia with minimal effects on feto- maternal well being. Although most patients undergoing caesarean section are young and healthy, they represent a high risk group of patients. Either of general and spinal anaesthesia is not ideal for caesarean section because each has advantages and risk to both mother and foetus. However the aim of anaesthetist is to choose the method which is safest and most comfortable for the mother, least depressive to the new born and which provides optimal working conditions for obstetrician1. Apgar score is the best parameter to assess the immediate condition of the baby.2,3 It is the first non invasive test done to the new born after birth. It is a bedside clinical method to assess the health of the new born immediately after birth and to determine the need of any resuscitative measures. The scores are taken at 1 and 5 minutes after birth. Of the two scores, the 5 minutes score is regarded as the better predictor of survival whereas 1 minute score has the value in assessing the effects of different drugs given to the mother during caesarean section. We conducted a randomized prospective comparative study to see the effects of general versus spinal anaesthesia in elective caesarean sections on Apgar score at 1 and 5 minutes.
METHODS After obtaining institutional ethic committee approval, this study was conducted in SMGS Hospital Government Medical College Jammu and Govt Hospital Sarwal Jammu over a period of 6 months. A total of 90 healthy full term pregnant patients presenting for elective lower segment caesarean section were chosen. Informed written consent was taken from all selected patients. Mother having PIH, gestational or pre pregnancy diabetes mellitus and morbid obesity (BMI > 40) were excluded from the study. Foetal factors for exclusion were antenatally diagnosed congenital malformations and small for date babies. Patients were divided into 2 groups. Group 1 comprised of 45 patients who received general anaesthesia Group 2 also comprised of 45 patients who received spinal anaesthesia History was taken from all patients including age, parity, duration of pregnancy and any complicating maternal history. Pre anaesthetic checkup was done which included BP measurement, airway assessment and cardiorespiratory examination. Method of general anaesthesia: A 18gauge intravenous canula was fixed. Premedication was done with injection ranitidine and metoclopramide. Patient was preoxygenated for 3 minutes. Induction was done with Inj Propofol 2.5 mg/kg and inj succinylcholine 1.5mg/kg. After endotracheal intubation 50% oxygen with nitrous oxide and 0.8% isoflurane inhalation was given. General anesthesia was maintained with non depolarising muscle relaxant Atracurium 0.5mg/kg. After delivery i/v syntocinon 10 units was given as a single dose and 10 units were added to the iv infusion. IV diclofenac 75 mg was given for analgesia to every patient after delivery. To reverse the effect of non depolarising muscle relaxant inj Neostigmine 0.05mg/kg and inj Glycopyrrolate 0.008mg/kg was given. Method of spinal anesthesia: After securing iv line patient was placed in sitting position and space between 3rd and 4th lumbar spine was identified and marked. After taking all aseptic measures, lumbar puncture was done with 25 gauge spinal needle and hyperbaric Bupivacaine 0.5% 2.5ml (12.5mg) was administered in one minute. Immediately after injection patient was placed in supine position with wedge under right hip for left uterine displacement. Monitoring was done for pulse, NIBP, oxygen saturation, ECG and urinary output. Following parameters were recorded during each caesarean section: Time of induction, time of incision to skin, time of incision of uterus and time of delivery of baby. Apgar score of all neonates was recorded by paediatrician attending the delivery. Apgar scores were recorded at 1 minute and 5 minutes after delivery. Birth weight of every baby was recorded. Apgar score of every baby was assessed as per the Apgar score chart shown below (Table 1).
Table 1: Apgar Score
Data was assessed using SPSS software. Age of mother and weight of mother and baby were expressed as mean + SD. Student t test was applied to compare the continuous variables and the mean of both groups. All data was presented as tables and figures. A p-value of < 0.05 was considered significant.
RESULTS The two groups of expectant mothers were comparable in terms of age, weight, preoperative mean arterial pressure and gravid status. The birth weight of newborn baby was also comparable in both the groups (Table 2).
Table 2: Demographic Characteristics of Study Population
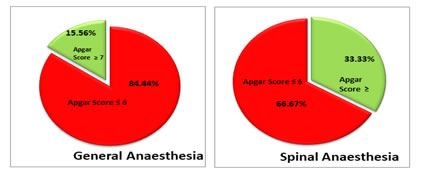
Out of 45 patients who received general anaesthesia, 38 patients (84.4%) gave birth to babies having Apgar score less than or equal to 6 at one minute after birth and the remaining 7 babies (15.5%) had APGAR score of more than or equal to 7. 37 babies with low Apgar score at 1 minute were resuscitated and had improved by 5 minutes with Apgar score of more than or equal to 7. Only 1 patient continued to have low APGAR at 5 minutes as well. Out of 45 patients who received spinal anaesthesia only 15 (33.3%) patients gave birth to babies having APGAR score less than or equal to 6 at one minute. Out of these 15 patients only 1 baby continued to have Apgar score less than or equal to 6 even after resuscitation at 5 minutes after birth (Table 3).
Table 3: Apgar Score at 1 minute and type of Anaesthesia
All babies who had Apgar score less than or equal to 6 at 5 minutes in both the groups were shifted to NICU for further management. It was observed that there is a statistically significant difference (p-value < 0.05) in Apgar score at 1 minute of babies born through LSCS under general and spinal anesthesia. Babies born through LSCS under general anesthesia were 11 times more likely to have Apgar score less than or equal to 6 at one minute as compared to babies born under spinal anesthesia (Odds Ratio 11) (Table 3) (Figure 1).
Figure 1: Apgar score at 1 Minute One baby in both the groups continued to have Apgar score of less than or equal to 6 at 5 minutes which is statistically insignificant. (Table 4) Table 4: Apgar score at 5 Minutes and type of Anaesthesia
DISCUSSION The choice of anaesthesia most appropriate for a caesarean section depends on many factors such as urgency of the situation and maternal medical condition. With better understanding of materno-fetal conditions, risks and benefits of different types of anaesthetic techniques have evolved. Given that the principal purpose of a caesarean section is to deliver a baby in as good or better condition than when the decision to operate is taken, it appears logical to examine critically the influence of the choice of anaesthesia on the neonatal outcome4. The Apgar score is a practical method of systematically assessing newborn infants immediately after birth to help identify those requiring resuscitation and to predict survival in neonatal period. The 1 minute Apgar score may signal the need for immediate resuscitation and 5minute score may indicate the probability of successfully resuscitating an infant. A low score may be due to a number of factors including drugs given to the mother during labour and caesarean section5 We conducted a study to compare the neonatal outcome in mothers receiving general versus spinal anaesthesia and observed that 84.4% of patients receiving general anaesthesia had babies with Apgar score less than or equal to 6 at 1 minute as compared to 33.3% of patients who received spinal anaesthesia. Similar results were seen by Hassan et al6 and Aftab Imityaz et al7. They observed in their study that Apgar score was significantly lower in patients receiving general anaesthesia as compared to spinal anaesthesia at 1 minute, but at 5 minutes Apgar score improved in most of the patients. Delivery of the baby by caesarean section has become increasing common and both general and spinal anaesthesia have certain advantages and disadvantages but regional anaesthesia has become the preferred technique because general anaesthesia is associated with higher maternal mortality and foetal depression.8 Internationally an obstetric anaesthesia guideline recommends spinal and epidural anaesthesia over general anaesthesia for most caesarean sections.9,10 This subject has been studied by many investigators over the years. Some have shown no difference in Apgar scores between the groups while others reported lower Apgar scores and worse outcomes with the use of general anaesthesia11 Apgars12 was amongst the first to report that the babies delivered by caesarean section under spinal block were in general more vigorous at birth than those whose mothers had cyclopropane. Several workers report a marginal improvement in 1 minute Apgar scores in babies delivered by LSCS under epidural block13-15, but others have found no difference.16,17 Krishnan et al studied two groups of patients, one received general anaesthesia and other spinal anaesthesia and found that no significant difference was seen in the mean 1 minute Apgar scores in the two groups. However more babies of the general anaesthesia group appeared depressed soon after birth needing free flow of oxygen and bag/mask ventilation18. Inhalational agents necessary for general anaesthesia could depress the newborn and in our study 1minute Apgar scores reflected the same effect. So we conclude that there is a significant difference between the effects of general anaesthesia and spinal anaesthesia on Apgar score of newborn babies at 1 minute after birth of full term neonates born by elective LSCS. The present study also revealed that the difference in Apgar score at 5 minutes after birth in two groups is statistically insignificant. We suggest that spinal anaesthesia should be preferred over general anaesthesia for LSCS unless otherwise contraindicated.
REFERENCES
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.