 Home
Home
|
Table of Content - Volume 18 Issue 1 - April 2021
A study on correlation between gestational age and foot length measurements
Narendra K S1*, Pagadpally Srinivas2
1Assistant Professor, 2Resident, Department of Paediatrics, Vinayaka Mission Medical College, Karaikal, Pondicherry, INDIA. Email: narendrak@yahoo.com
Abstract Background: The comparison with determination of CHL and birth weight, the foot length measurement is more convenient in preterm sick neonates, in special care units without disturbance to such infants. It could also be useful in deriving the surface area more accurately than from birth weight alone for the calculation of drug doses and fluid requirements in preterm. Methodology: All the singleton live born babies born in the hospital were examined with in 48 hours of birth. Gestational age was calculated by enquiring into 1st day of mothers last menstrual period and will be subsequently confirmed by New Ballard Score.If any disparity of more than 2 weeks between gestational age by enquiring LMP and by NBS, were excluded from the study. Results: The mean foot length of the babies analyzed was 8.03 cm, with the SD of 0.80 cm. It was found that foot length was correlated well with the gestational age. Conclusion: In the derived normogram based on foot length and gestational age it was observed that there is a linear relationship of the foot length with increasing gestational age. Keywords: Gestational Age, Foot Length Measurements, normogram
INTRODUCTION In preterm, the foot length correlated with all three indices i.e. CHL, HC and birth weight. Foot length has a positive linear correlation with other body measurements in a neonate and has the highest correlation in preterm babies with CHL.1 When applied to neonates it was found to correlate with 95% of the babies. Hence, because it is easy, requiring less handling and less disturbing to the neonate, foot length is a better screening tool. Very few studies have been done on determining the usefulness of foot length. Significant relationship between foot length and other parameter has been observed in these studies.2 The highest correlation in term small for gestational age and term AGA babies for foot length was with HC indicating that foot length and HC are affected in a similar fashion in term neonates.3 The comparison with determination of CHL and birth weight, the foot length measurement is more convenient in preterm sick neonates, in special care units without disturbance to such infants. It could also be useful in deriving the surface area more accurately than from birth weight alone for the calculation of drug doses and fluid requirements in preterm. Hence foot length is a new and potentially useful measurement in the neonate.4
METHODOLOGY All the singleton live born babies born in the hospital were examined within 48 hours of birth. Gestational age was calculated by enquiring into 1st day of mothers last menstrual period and will be subsequently confirmed by New Ballard Score. If any disparity of more than 2 weeks between gestational age by enquiring LMP and by NBS, were excluded from the study. Their gestational ages ranged from 29 to 42 weeks. As there were few babies in less than 30 weeks gestation they were grouped together. Newborns were subjected to the following anthropometric measurements within 48 hours of birth by standard techniques. Birth weight: Babies were weighed naked immediately after birth on lever actuatedweighing scales to the nearest 50 g. The weighing machine was checked periodically by known standard weights. Crown heel length: The baby was placed supine on an infantometer. The head is heldfirmly in position against a fixed upright headboard. Legs are straightened keeping feet at rights to legs with toes pointing upwards. A free footboard is brought into firm contact with the baby's heels. Length of the baby is measured from a scale, which is set into the board. Head circumference: A flexible non-stretchable fiber glass tape was used. The headcircumference in the largest dimension around the head (the occipito-frontal circumference) was obtained with a tape placed snugly above the ears. The tape is placed over the mid forehead and is extended circumferentially to include the most prominent portion of the occiput .The measurement was taken to the nearest 0.1cms. Foot length: A wooden scale was used with 0.1cm division and it was fixed againstthe foot and the distance from the heel to the tip of great toe of the left foot was measured to the nearest of 0.1cm, after straightening the foot. INCLUSION CRITERIA All the singleton live born babies born in hospital were included in the study. EXCLUTION CRITERIA
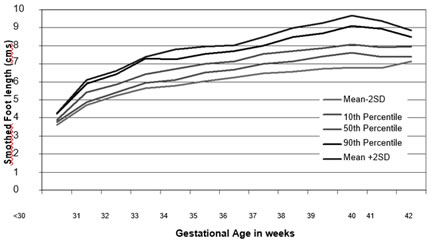
RESULTS The mean foot length of the babies analyzed was 8.03 cm, with the SD of 0.80 cm. It was found that foot length was correlated well with the gestational age. (r = 0.523, p < 0.0001) In the derived normogram based on foot length and gestational age it was observed that there is a linear relationship of the foot length with increasing gestational age. There is increase in the foot length with the increasing gestational age, which started declining after 40 weeks gestations.
Table 1: Foot length
Graph 1: Shows the normogram of foot length with 10th, 50th, 90th percentiles and mean ± 2SD
DISCUSSION Growth is defined as an increase in size over time, and documentation of increasing size thus requires two or more serial measurements. During fetal life, however, serial measurements are feasible only with ultrasound and have not proved to be sufficiently valid or precise (ultrasound estimation of fetal weight has a high coefficient of variation) to serve as a standard for assessing fetal growth as (WHO Tech report series 854) 5 Moreover, ultrasound measurements are not truly anthropometric. There is of course an inherent limitation in estimating intrauterine growth from the weight of infants who have been born at various gestational ages. The sample has an undeterminable bias because premature birth itself is probably related to unphysiological states of variable duration in either mother or fetus. Since exact size of fetuses that remain in utero cannot be measured, the curves presented here in are submitted with reservation as estimates of intrauterine growth Measured carefully from the heel to the tip of the longest toe also correlates with gestational age in appropriately grown infants. The foot measures 4.5 cm at 25 wks and increases by 0.25 cm/wk until term.6 The average foot length of a term neonate baby is 7.3-7.9cms.7 Foot length in a neonate is another useful measurement to assess birth weight of a baby quickly. It also corresponds well with gestational age, ChC and HC.8 It can be used to calculate body surface area and drug doses. CHL measurement is more disturbing the neonates, especially to the preterm under intensive care. Flexor posture of a term baby also leads to difficulty in measurement. In such situation FL measurement gives alternate method. In one study done, a formula to determine CHL from foot length has been derived in neonates.
CONCLUSION There is increase in the foot length with the increasing gestational age, which started declining after 40 weeks gestations
REFERENCES
Policy for Articles with Open Access: Authors who publish with MedPulse International Journal of Pediatrics (Print ISSN: 2579-0897) (Online ISSN: 2636-4662) agree to the following terms: Authors retain copyright and grant the journal right of first publication with the work simultaneously licensed under a Creative Commons Attribution License that allows others to share the work with an acknowledgement of the work's authorship and initial publication in this journal. Authors are permitted and encouraged to post links to their work online (e.g., in institutional repositories or on their website) prior to and during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work.
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.