 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 9 Issue 1 - January 2019
A study of clinical profile of patients with cerebral palsy
Jeetendra Kumar
Senior Resident, Dept. of Pediatrics, Vardhman Institute of Medical Sciences, Pawapuri, Bihar, INDIA. Email: jeetendrakr98@gmail.com
Abstract Background: Cerebral Palsy is combined disorder of movement, posture, and motor function and may be associated sensory, neurological and musculoskeletal complications. It is a permanent condition attributed to nonprogressive disturbances that occurred in the developing brain. Objectives: To study the clinical profile of children with cerebral palsy. Material and Methods: This study was done at paediatrics department at tertiary care center. Total of 50 cases with cerebral palsy coming to OPD were selected after fulfilling inclusion criterias. Results: 2-5 age group was found to be most vulnerable 42% in this study. Males were in majority 78% of cases, spastic palsy 83% was most common palsy seen in this study. Diplegic spastic palsy 60% was seen most commonly. Birth asphyxia 78% was most common etiological factor seen in this study. Conclusions: CP incidence can effectively be reduced by raising the quality of health education, pregnancy monitoring, delivery care and neonatal intensive care units. Key Word: Cerebral Palsy, Spastic palsy, Diplegic palsy, Birth asphyxia
INTRODUCTION Disabled children are of great concern to a family as well as to the society.1 Cerebral palsy (CP) is the most common type of motor disability in childhood.2 It is found that 10% of the global population has some form of disability from different causes; in India, it is 3.8% of the population. Nearly 15-20% of physically disabled children are affected by Cerebral Palsy.3 Its incidence in India around 3 cases per 1000 live births; however, being a developing country, the actual figure may be much higher. The prevalence and pattern of Cerebral Palsy varies between different geographical regions, probably because of different etiological factors and different classifications used.4 The prevalence was significantly higher in boys than girls (male/female ratio 1.4:1).5 The motor disorders of Cerebral Palsy are often accompanied by disturbances of sensation, perception, cognition, communication and behavior, by epilepsy, and by secondary musculoskeletal problems.6 Cerebral palsy (CP) is caused by abnormal development of the brain or damage to the developing brain that affects a child’s ability to control his or her muscles. There are several possible causes of the abnormal development or damage. People used to think that CP was mainly caused by lack of oxygen during the birth process. Now, scientists think that this causes only a small number of CP cases. Other causes are LBW, preterm births, jaundice, infections in pregnancy, injuriesetc.7,8 The topographic classification of CP is monoplegia, hemiplegia, diplegia and quadriplegia; monoplegia and triplegia are relatively uncommon. There is a substantial overlap of the affected areas; diplegia is the commonest form at 30% – 40%), hemiplegia is 20% – 30%, and quadriplegia accounts for 10% – 15%. In an analysis of 1000 cases of CP from India, it was found that spastic quadriplegia constituted 61% of cases followed by diplegia 22%.3 Spastic CP is the commonest and accounts for 70%-75% of all cases, dyskinetic for 10% to 15% and ataxic for less than 5% of cases.9 Another classification, GMFCS, describes the functional characteristics in five levels, from I to V, level I being the mildest in the following age groups: up to 2 years, 2– 4 years, 4 – 6 years and 6 – 12 years. For each level, separate descriptions are provided.10 Since CP is a continuing problem, it is important to study and explore the causes and the newer aspects of the condition for proper understanding and management.11 There are less number of studies done on cerebral palsy in this study area so we undertook this study to see clinical profile of cerebral palsy in children of this area.
MATERIAL AND METHODS This study was done at paediatrics department at tertiary care center Vardhman Institute of Medical Sciences. Total of 50 cases with cerebral palsy coming to OPD formed the sample size for after approval from Institutional ethical committee. The cases were classified based on the modified Minear’s classification.12,13 A preformed proforma was used for collecting all the relevant history from either parents or caregivers after taking consent. Complete anthropometric measurement, complete paediatric assessment was done. Neuromusculoskeletal examination were carried out in all cases. All necessary investigation were done. Data was entered into Microsoft excel and analyzed using SPPS software.
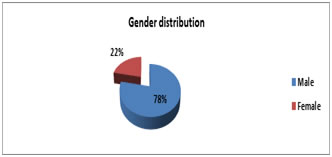
RESULTS Total 50 patients between 5 months to 15 years of age were included in this study. 78 % male and 22% were female.
Table 1: Distribution as per age at presentation
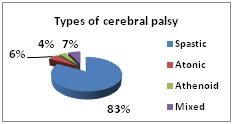
Most children (44%) are from 2 to 5 years of age category while 30% belonged in less than 2 years category. Overall mean age was found to be 4.5 years. Males fromed 78% while females formed 22% with M:F ratio of 3.5:1. Diagram 2: Distribution of the patients as per the clinical types
83% cases belonged to spastic type and next most type was mixed with 7% cases.
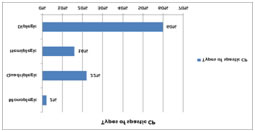
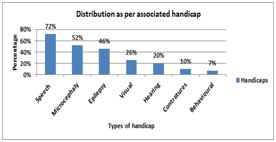
Diagram 3: Distribution as per various types of spastic CP Most common spastic type was found to be diplegic 60%, next common was quadriplegic with 22% cases. Diagram 4: Distribution of associated handicaps Most common handicap seen was speech defects 72%, next was microcephaly with 52% cases.
Table 2: Distribution as per intra natal , pre natal and post natal etiological factors
Most common intra natal etiological factor was found to be maternal age with 18% cases. Most common factor in perinatal category was severe asphyxia seen in 78% cases, while in post natal group hyperbilirubinemia 12% was seen as most common factor in cerebral palsy cases.
DISCUSSION This was a cross sectional study done on 50 cerebral palsy cases in a tertiary care center. Most children (44%) belonged to 2 to 5 years age category while 30% belonged in less than 2 years category. Overall mean age was found to be 4.5 years in this study. Singhi PD et al3 in their study males formed 67.5% of all cases, Srivatsava VK et al14 study said males were 65.1%. Similarly Reddy B et al15 and Laisram N et al16 study had almost similar male dominance as of our studies. In this study we found 83% cases belonged to spastic type and next most type was mixed with 7% cases. Kumar R et al11 reported 75% cases with spastic palsy. Spastic palsy in 52%, Atonic in 28%, Mixed were 20% in a study done by Bendale AG et al,17 Das Net al 18 found Spastic type predominantly in (80%) cases, all these studies had similar findings as our study. Most common spastic type was found to be diplegic 60%, next common was quadriplegic with 22% cases in this study. Kumar R et al11 reported similar findings with % cases with spastic palsy, In contrast to our findings Gowda et al19 have reported 16% cases of spastic diplegia. In present study the most common handicap seen was speech defects with 72%, next was microcephaly with 52% cases, epilepsy in 46% and visual defects in 26% cases. Fidan et al20 reported similar hearing defects as our study. Das N et al18 and Kumar R et al11 reported hearing defects in 7% and 15% cases respectively. Kumar R et al11 reported microcephaly in 25% both these findings were in accordance with our study. Sharma P et al21 reported ocular defects in 35.8% which was supporting our study. Most common intra natal etiological factor was found to be maternal age with 18% cases. Das N et al18 also concluded similar results. Wu et al22 and Thorngren-Jerneck et al23 reported that maternal age over 35 years increased the risk of Cerebral Palsy by twice. Das N et al18 reported 15% cases with prematurity and 36% LBW cases, similarly Gowda et al19 found 15% cases of prematurity and 30% cases with low birth weight. Both these studies had similar results as our study with asphyxia seen in 78% and LBW in 40%. In present study postnatal infections counted for 16% overall cases. Similar was reported by Das N et al,18 sharma P et al21 and Gowda et al19 with 11%, 15% and 12% cases presenting with infections postnatal.
CONCLUSION We found that males were forming majority and it was observed in this study that perinatal factors were a major risk factors in development of CP. We can say that CP incidence can effectively be reduced by raising the quality of pregnancy monitoring, delivery care and neonatal intensive care units.
REFERENCES
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.