 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 9 Issue 1 - January 2019
A study of clinical profile and prevalence of Noro virus in acute Diarrhoea among children attending a tertiary care hospital
K Nagendra Prasad1, S Sri Krishna2*, Ajay Kumar Reddy Bobba3, N Partha Sarathy4
1Associate Professor, Department of Paediatrics, Santhiram Medical College, Nandhyal, Andhra Pradesh, INDIA. 2Associate Professor, Department of Paediatrics, Apollo Medical College, Hyderabad, Telangana, INDIA. 3Assistant Professor, 4Professor and HOD, Department of Community Medicine, Alluri Sitarama Raju Academy of Medical Sciences, Eluru, Andhra Pradesh, INDIA. Email: ajay_reddy52420@yahoo.com
Abstract Background: Diarrhoea is defined as the passage of three or more liquid stools within 24hrs, however it is the recent change in consistency and character of the stools rather than number of stools that is the more important feature. Aims and Objectives: To study the prevalence of acute gastroenteritis due to Noro virus in children <12years. To study the clinical profile of gastroenteritis due to NOROVIRUS in children. Materials and Methods: Type of study: Cross sectional. Type of Sample: Stool samples from children < 12years with acute gastroenteritis. Study Duration: The study was conducted from March 2018 to June 2018. Conclusion: Noro virus is one of the contributors, emerging recently as a cause of gastroenteritis in children < 12 years of age. There is a need for larger and long term studies in future. Further studies will fill the gap of undiagnosed aetiology of diarrhoea. Key Word: Noro virus, acute gastroenteritis.
INTRODUCTION Diarrhoea is defined as the passage of three or more liquid stools within 24hrs, however it is the recent change in consistency and character of the stools rather than number of stools that is the more important feature.1 Gastroenteritis a major cause of childhood mortality and morbidity worldwide, especially in developing countries. About 1.8million deaths are estimated to result each year as a consequence of diarrhoeal disease in under five children.2 It accounts for 20.3% of all deaths among children under five in India.3. Children under five years of age in developing countries experience the highest rates of illness and deaths due to diarrhea.4 The magnitude of the problem in a given population largely depends upon socio-economic and physiologic factors like overcrowding, poor hygiene, polluted water, poor sanitation, under nourishment and inadequate public health facilities. Transmission is primarily through faeco –oral route, either by consumption of faecal contaminated food or water or by direct person to person spread. Diarrhoea can be caused by a variety of different pathogens including bacteria, virus and parasites. Among the viruses, rotavirus has been extensively studied and is responsible for 44% of GE cases. After Rotavirus, It has been increasingly recognized that Human Calciviruses comprising Noroviruses and Sapoviruses are important causes of gastroenteritis in both outbreak and non-outbreak settings.5 Since the application of molecular assays, Norovirus have been well documented as the leading cause of epidemic gastroenteritis in all age groups across the world 6. Norovirus, previously known as Norwalk virus is a single stranded RNA virus. It is highly contagious can tear through crowded spaces. Young children, elderly and immune compromised persons are more susceptible. Infection by Norovirus is characterized by damage to the microvilli in the small intestine. The incubation period for Norovirus associated GE in humans is usually between 24 to 48hrs.but cases can occur within 12 hrs of exposure7. The most common symptoms being nausea, vomiting, diarrhoea and stomach cramps (commonly known as Stomach flu). Identification of the virus can be best made from stool samples taken within 48 to 72 hour after onset of symptoms. Good results can be obtained by using RT –PCR on samples taken as long as 5 days after onset of symptoms. Sometimes Virus can be found in stool samples taken as long as 2 weeks after recovery. Water can be tested for Noro viruses by using RT – PCR to detect virus when large volumes of water are processed through specially designed filters. Enzyme linked Immune Sorbent Assay (ELISA) have been developed for the diagnosis of Norovirus.8 The well-established Enzyme Immuno-assay kit is the RIDASCREEN. A new kit is the RIDAQUICK. Treatment modalities include Oral rehydration therapy with ORS or IV Fluid therapy depending upon the severity of Dehydration.
MATERIALS AND METHODS Type of study: Cross sectional Type of Sample: Stool samples from children below 12years with acute gastroenteritis. Sample size (n): 125 Duration The study was conducted from 1/3/18 to 30/6/18 Exclusion Criteria: Children below 2 months and above 12 years. Children with dysentery, persistent diarrhoea. Specimen Collection: Samples were collected from children reporting to Hospital with acute Diarrhoea. Both outpatient and admitted children were included in the study. After an informed consent from the patient or guardian of the child, a short epidemiological information form and clinical questionnaire was filled in and specimens were collected. The form includes demographic details along with details of symptoms, home treatment plan and knowledge of feeding and ORS therapy. Stool samples were collected into a sterile wide mouthed container within 24hrs of reporting to hospital. The stool samples were made homogenous by vortex if liquid or by drop by drop dilution with water until liquid and then vortex. Two aliquots of 1ml were placed in CRYO S screw cap tubes and the remainder in the wide mouth plastic container. The aliquots and remainder of homogenized sample was frozen at -20o C until further need. Test Kits are Ridascreen Novovirus, Ridaquick Norovirus Sample preparation: 100ml of liquid stool was suspended in 1ml of dilution buffer, these were homogenized using vortex and let to settle for 6 minutes. The supernatant was used in the assay. RIDASCREEN EIA for NOV Ag detection samples were processed by a setup of 30 samples at a time and allowing them for replication. Further steps are followed according to manufactures protocol. After 3 incubations for about 105min, final plate was available for OD450nm reading. Sample was considered positive if OD 450nm value is 10% or more above the cut-off point and negative if OD 450 reading fall 10% or more below out off point.
Rapid test for Norovirus Rida Quick: The samples for this assay were the ones prepared for RIDASCREEN. The cassette with sample was incubated for 15min at room temperature as per manufacturer protocol. Results were read within first 3 minutes of adding the substrate to the reaction window. Cassettes with only blue line on C side visible were NOV negative. The cassettes with a blue line on the C side and T side were NOV positive
RESULTS AND ANALYSIS The total number of cases studied were 125. Epidemiological data: The age profile of diarrhoea cases shows a fall as age increases. 45.7% of cases in < 1yr age, 34.7% of cases in children between 1-4years of age, 14.4% among 5-8years of age and 5.08% among 8-12 years of age. About 53.3% are male children and 46.6% are female children.
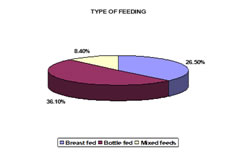
In children < 2years, 26.5% were breast fed, 36.1% were bottle fed and 8.4% were on mixed feeds. In children < 2years (n = 83) Figure 2: Type of Feeding
Regarding the knowledge of hygiene (hand washing with soap before preparing food, before feeding children, after work etc) among mothers, 25.42% never washed their hands with soap, 60.16% used soap occasionally and only 14.4% used soap always. Figure 2: Washing Hands with Soap
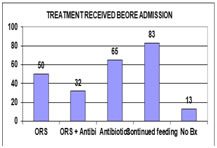
Diarrhoea is associated with loss of nutrients. So there is a need for continuous feeding during diarrhoea. 70.3% of mothers continued to feed during diarrhea. Regarding the treatment used for diarrhoea before admission in Hospital, 42.37% used ORS, 27.11% used both ORS and Antibiotics 55.08% were on antibiotics and 11% took no treatment at all. Figure 3: Treatment Received Before Admission
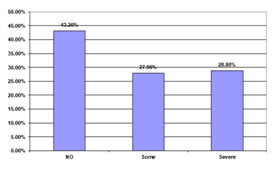
About 43.2% presented with no dehydration, 27.96% presented with some dehydration and 28.8% presented with severe dehydration. Figure 4: Regarding The Severity Of Dehydration
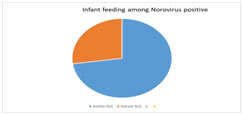
Out of 125 cases, 11 cases were Noroviruses positive i.e., 8.8% of cases were Norovirus positive. These 11 cases were between 7months to 1 ½ yr of age, of which 8 of them were bottle fed and 3 were breast fed. 8 children had no dehydration and 3 had moderate dehydration. Figure 5- Norovirus cases and infant feeding DISCUSSION The age profile shows a fall in the number of diarrhoea cases as the child’s age increases which is explained by improved personal hygiene and less susceptibility to infection as age increases. This is supported by the study done by Yehuda et al9 which showed the age of the child was the most important risk factor, with mean no of episodes of acute diarrhoea per 12 child months was 2.28 in 0-2years, 0.44 in 2-6years, 0.12 in 6-13years and 0.03 in 13-18years old. More no of boys are affected than girls. Among children < 2years with GE, it was found that 36.1 were bottle fed, 26.5% were breast fed and 8.4% were given mixed feeds. Bottle feeding is an important risk factor for GE. A breast fed baby is 14.2 times less likely to die of diarrhoea (IAP) as it contains a number of protective factors (which include immunoglobulin, mainly secretory IgA, macrophages, lymphocytes, lysozyme, bifidus factor, interferon and other protective substances). In a study by V Kumar et al,10 the morbidity from diarrhoea was higher in bovine, bottle fed group than breast fed. In a study by Cesar et al,11 Brazil, the risk for infants who did not receive breast milk was 14.25 times higher and those who received mixed feeding the risk was 4.2 times higher. In this study, it was found that only 14.5% use soap to wash hands regularly before preparing food, before feeding etc. 60.16% used soap occasionally for hand washing and 25.42% never washed their hands with soap, so there is a need for emphasis on hand washing. In a RCTrial on effect of intensive hand washing on childhood diarrhoea in Pakistan by Luby et al (2004), the incidence of diarrhoea in older children decreased by 53% compared to controls and by 39% in infants.12Diarrhoea is associated with nutrient losses. Food is often withheld from the child by the mother because of an erroneous belief that rest to the bowel promotes early recovery. Since children with diarrhoea may develop protein energy malnutrition it is desirable to continue feeding in acute diarrhoea and the diet should be digestible and nutritionally balanced. Presence of nutrients in the gut hastens recovery of intestinal epithelium because food in the intestine stimulates rapid cell turnover and renewal of intestinal lining. In this study, 70.3% of mothers continued to feed their children during diarrhoea. About the treatment given to the child before admission to hospital, it was found that among children brought with diarrhoea, 55.08% were started on antibiotics, only 42.37% received ORS, 27.11% received both ORS and antibiotics and 11% received no treatment at all. According to the diarrhoea disease control programme, ORS is the treatment protocol for diarrhoea. ORS is appropriate for both prevention and treatment of dehydration in diarrhoea. Only 42.37% used ORS in this study. Antibiotics are not indicated in diarrhoea as a large majority of cases of diarrhoea are caused by viruses or toxigenic bacteria and there is little evidence of inflammation of gut mucosa. Their indiscriminate use leads to emergence of resistant strains of harmful bacteria and eliminates resident flora which protects the gut. In this study it was found that 55% of children were put on antibiotics before coming to hospital. The National Family Health Survey (1992-3) revealed that 42.7% of mothers knew about ORS and 25.9% had ever used them. ORS use rates in children who suffered from diarrhoea varied from 8.3% in Rajasthan to 50.1% in West Bengal. This is a reminder that we still have to reach more than half of households.13 In this study, the contribution of Nov to GE is 8.8%. Among those positive, all are under 1 ½ year of age. 8 had no dehydration, 3 had mod dehydration. The earlier studies done in India at Pune by Preeti Chabra et al14 showed 11.9% positivity. There was a predominance of GII4 along with cocirculation of GII-1, GII– 2, G-IIb. Clinical severity score showed severe disease in majority (70.8%) and moderate disease in 29.2%. Study conducted in Vellore, South India showed 19.4% positivity for human Caliciviruses in hospitalized children, 15.1% were positive for NOVs and 5% for SaVs GII3 was the most frequently identified genotype followed by GII – 1 and GII – 4 in equal proportion.15 Systematic literature review of Role of Noroviruses in Sporadic Gastroenteritis by Manish M Patel et al,16NoVs accounted for 12% of severe gastroenteritis among children < 5years of age and 12% of mild and moderate diarrhea cases among persons of all ages. In a report from Thailand, 12% of stool specimens were positive for NoVs (Hansman et al).17
SUMMARY AND CONCLUSION NOROVIRUS is one of the contributors, emerging recently as a cause of gastroenteritis in children < 12 years of age. There is a need for larger and long term studies in future. Further studies will fill the gap of undiagnosed etiology of diarrhea.
REFERENCES
|
|

 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.