 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 9 Issue 2 - February 2019
A study of prevalence and factors associated with overweight and obesity in school children
Jeetendra Kumar1, Avinash Kumar Sahay2*
1Senior Resident, 2Associate Professor, Department of Paediatrics, Vardhman Institute of Medical Sciences, Pawapuri, Bihar, INDIA. Email: jeetendrakr98@gmail.com
Abstract Background: Overweight and obesity are by definition, abnormal or excessive fat accumulation that may impair health. The prevalence of obesity is increasing worldwide in almost every country in all the age groups. Obesity in children is pf more concern because these are future risk factors for development of most of the noncommunicable diseases. Aim and objective: To study the prevalence and factors associated with overweight and obesity in school children. Methodology: total 1100 school going children were studied. Data collected with pretested questionnaire. Data collected was sociodemographic data, anthrpometric measurements and various risk factors like watching TV, less physical activity and intake of junk food. Data was analysed with appropriate statistical tests. Results and discussion: Prevalence of overweight and obesity among study population was 8.72% and 1.28% respectively. Overweight and obesity was significantly associated with higher SES, watching TV/computer >2 hrs per day, use of vehicle for commuting to school, junk food frequency > 2 per week and physical activity less than 30 min. per day. Key Word: overweight, obesity.
INTRODUCTION Disease pattern is changing worldwide. This is particularly true in low and middle-income countries that form the major chunk of global population. The emerging epidemics of obesity, cardiovascular disease and diabetes form the crux of this phenomenal change. Among these entities, obesity has become an epidemic causing serious public health concern and contributes to 2.6 million deaths worldwide every year.1 Obesity is associated with an increased risk of morbidity and mortality as well as reduced life expectancy. The last two decade of previous century have witnessed dramatic increase in health care cost due to obesity and related issues among children and adolescents.2 For children and adolescents, overweight and obesity are defined using age and sex specific normograms for body mass index (BMI). Children with BMI equal to or exceeding the age-gender-specific 95th percentile are defined obese. Those with BMI equal to or exceeding the 85th but are below 95th percentile are defined overweight and are at risk for obesity related co-morbidities3. It has been estimated that worldwide over 22 million children under the age of 5 are obese, and one in 10 children is overweight.4 Globally the prevalence of childhood obesity varies from over 30% in USA to less than 2% in Sub-Saharan Africa. Indian data regarding current trends in childhood obesity are emerging. Available studies of Delhi and Chennai has shown the prevalence of 7.4% and 6.2% respectively.5,6A study conducted among adolescent school children in South Karnataka has shown the prevalence of overweight and obesity to be 9.9% and 4.8% respectively.7 Aetiopathogenesis of childhood obesity is multifactorial. Interactions between genetic, neuroendocrine, metabolic, psychological, environmental and socio-cultural factors are clearly evident in childhood obesity.8There is evidence stating that individual`s eating and physical activity behaviors are heavily influenced by surrounding social and physical environmental contexts both for adults and children. Television viewing and other sedentary activities have also been related to childhood obesity. Unfortunately this habit is growing exponentially in developing countries9 There are numerous psychological, physical and economic consequences of obesity. Childhood obesity affects self esteem and has negative consequences on the cognitive and social development.10Conditions such as type 2 diabetes mellitus, hypertension and hypercholesterolemia, which were noted primarily in adults, are becoming more common among children with the increase in the prevalence of obesity.11 Due to difficulty in the treatment of obesity in adults and the many long-term adverse effects of childhood obesity, prevention of childhood obesity has now been recognized as a public health priority.12With this backgroundin mind, the present study was undertaken to know the prevalence of obesity and its influencing factors in school children.
MATERIAL ANDMETHODS The study was done in 1100 school children in urban area. Inclusion criteria: 1. Children attending school in an urban area 2. Whose parents are willing to participate. Exclusion criteria: 1. Students absent on day of data collection 2. Whose parents not willing to participate 3. Children with severe diseases The study was approved by the Ethical Committee Permission was obtained from the authorities of local school. Teaching and administrative staff and students underwent prior orientation about the study. A valid written consent was obtained from parents after explaining study to them. Data was collected with pretested questionnaire. Data included various socio-demographic variables, influencing factors with respect tobesity. Anthropometric measurements were done. The time selected for undertaking the measurements was during the schoolworking hours. Anthropometric measurements included Weight, Height. The sociodemiographic data was filled by the parents. School children were sent to home with parental form one day prior to their interview and measurements. Children were classified into according to their BMI as obese, overweight, normal and underweight. IOTF(International Obesity Task Force) cut off points were used for classifying children into different classes. Data was analysed with appropriate statistical tests.
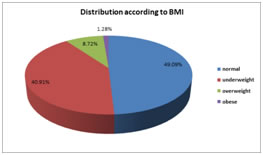
RESULTS Figure 1: Distribution of children according to BMI Total 1100 students were studied. Mean age of the children was 11.32±1.7 years. Age ranged from 9 to 14 years. 600 boys and 500 females were studied. Among 1100 students majority of the students were with normal BMI (49.09%). Almost 40% of the children were underweight according to BMI. Out of 1100 children 96(8.72%) were overweight and 14(1.28%) were obese according toIOTF(International Obesity Task Force). Thus prevalence of overweight and obesity among study population was 8.72% and 1.28% respectively.
Table 1: Association of risk factors in school children with their BMI
Table 1 shows association of various factors with BMI of children. It was observed that males predominate the females but the difference was statistically not significant. In age group majority of the students were in age group of 9-11 years but the difference was statistically not significant. Higher socioeconomic status was significantly associated with overweight and obesity among children (p<0.05) In case of obese children majority of the children were going to school by vehicle (11 out of 14). the difference between these groups is statistically significant (p<0.05). physical activity of >30 minutes is an protective factor for overweight and obesity. Majority of the children from overweight and obese group were having physical activity less than 30 minutes. TV/ Computer watching also affected the BMI of children. Children with TV/Computer watching time for more than 2 hrs per day have higher BMI than the normal one. This difference was statistically significant(p<0.05). We calculated junk food frequency per week among all children. Prevalence of overweight and obesity was significantly more in those children with junk food frequency more than 2 per week than those with less junk food intake(p<0.05).
DISCUSSION Mean age of the children was 11.32±1.7 years. 600 boys and 500 females were studied. Similar findings were observed in Premanath et al. 13 in Mysore, there were 54.5% were males and 46.1% were females Prevalence of overweight among study population was 8.72%. Similar results were found by Kapil et al.5(7.4%), AvulaLaxmaiahetal.14(7.2%), Kumar et al.15(5.74%). It was observed that prevalence of obesity was 1.28%. similar results were seen by Mishra A et al.16(2.8%), AvulaLaxmaiahet al.14(1.6%) and Bharati et al.17(1.2%) In our study the prevalence of obesity was more among male population ascompared to that in females It was also comparable with a study by Kapil et al.5males were more (8.3%) as compared to female (5.5%).Prevalence of overweight and obesity was more in 9-11year age group in our study. Similarily in a study by Kapil et al.5maximum prevalence of obesity was in the pubertal age group 10-12 years. The prevalence of obesity was found to be significantly associated with children of Upper Socio Economic Status than those of other class. Comparable findings were found in study by Marwah et al.18and Shabana etal.19 Use of motor vehicle was statistically associated with the prevalence of overweight and obesity. Similar results were found in a study by Avula Laxmaiah14in Hyderabad. Majority of the children from overweight and obese group were having physical activity less than 30 minutes. Similar findings were seen in S. Kumar et al.15(OR: 2, P< 0.001) and Kotian et al.7 (OR: 21.09 95% CI :2.77-166.8).Those who watch TV for more duration hadmore chance of getting obese or overweight as compared the other group. These findings were consistent with a study by Kuriyanetal.20(OR :19.6 p < 0.001) and Kotian et al.7(OR 7.3, 95%CI = 3.6-14.66).In present study it was found that Prevalence of overweight and obesity was significantly more in those children with junk food frequency more than 2 per week than those with less junk food intake(p<0.05). Study conducted by S Kumar et al.15inDavengere showed that eating junk food for >2 times perweek to be associated significantly with obesity( OR; 5.6p<.001) .
CONCLUSION Overweight and obesity was significantly associated with higher SES, watching TV/computer >2 hrs per day, use of vehicle for commuting to school, junk food frequency > 2 per week and physical activity less than 30 min. per day.
REFERENCES
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.