 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 5 Issue 2 - February 2018
Influence of glycaemic control on platelet count in type II diabetics in absence of vascular complications
Kazi Husna Abdul Naeem1, Mohammed Abdul Hannan Hazari2, Farisa Khatoon3*, Farah Bahmed4, Fariha Mohammedi5
1,5PG, 2Professor and HOD, 3Professor, 4Associate Professor, Department of Physiology, Deccan College of Medical Sciences, Hyderabad, Telangana, INDIA. Email: husnakazi008@gmail.com
Abstract Background: Diabetes mellitus (DM) has attained a state of a global emergency with increasing prevalence worldwide. Altered thrombocyte morphology, count and function have been reported with diabetics. The present study aimed at determining the variation in platelet count with degree of glycaemic control in Type 2 diabetes patients. Methods: A total of 200 subjects were enrolled in the study of which 100 had HbA1c < 6.5 and 100 had HbA1c > 6.5. Sample for glucose estimation and platelet indices were collected and estimation were carried out by the auto-analyzer. The statistical evaluation was done using SPSS version 22. Student t- test was used for comparison between two variables namely HbA1c and platelet count. Results: Mean Platelet count was found to be significantly higher in patients with type -2 diabetes mellitus with HbA1C > 6.5 in comparison to patients having HbA1c < 6.5.(p < 0.01) Conclusion: This study revealed a higher mean platelet count for diabetics with poor glycaemic control than for diabetics with good glycaemic control. However, platelet counts in both groups were within the normal reference range for healthy individuals. Platelet count with other platelet indices like Mean Platelet Volume and Platelet Distribution Width are simple, effective and cheap tests that may be used to predict vascular complications in type 2 DM. Key Words: Diabetes mellitus, mean platelet count, glycaemic control.
Diabetes mellitus (DM) is described as a constellation of metabolic diseases characterized by elevated blood glucose levels (hyperglycemia) which results from defects in insulin secretion, insulin action or both. It is a highly disabling disease, which can cause blindness, amputations, kidney disease, cardiovascular and cerebrovascular complications, among others, impairing the functional capacity and autonomy and individual quality of life. Diabetes mellitus has been labeled as a “Global emergency” now by the International Diabetes Federation. The prevalence of diabetes mellitus is increasing worldwide. In addition to the 415 million adults who are estimated to currently have diabetes, there are 318 million adults with impaired glucose tolerance, which puts them at high risk of developing the disease in the future. This number is expected to rise to as high as 615 million by the year 20401. According to statistics from International Diabetes Federation (IDF), India has more diabetics than many other nations of the world. Current estimates peg the number of diabetics in the country at about 62 million – an increase of over 10 million from 2011 when estimates suggested that about 50.8 million people in the country were suffering from the disease. Eighty percent of patients with diabetes mellitus die a thrombotic death. Seventy-five percent of these deaths is due to cardiovascular complications, and the remainder is due to cerebrovascular events and peripheral vascular complications2. Altered platelet function, impaired fibrinolytic activity and abnormal coagulation due to insulin resistance and /or metabolic derangements associated with diabetes seem to be the likely causes of increased vascular complications3. Several authors like Luscher et al4, Ferroni P et al5 and Colwell J et al6 have documented that increased morbidity and mortality in type 2 DM are associated with macro-vascular (cardiovascular diseases, stroke and peripheral arterial disease) and micro-vascular (nephropathy, neuropathy and retinopathy) complications due to platelet dysfunction. Also, an increased platelet counts and activity have been reported in diabetics as demonstrated by increase in GPsIIb/IIIa, 1b-IX, and 1a/IIa6,7, CD62 and CD63. Platelet count and mean platelet volume (MPV) are simple, effective and cheap tests that may be used to assess thrombotic potential in type 2 DM. This study aimed to establish variations in platelet count in type 2 diabetic patients with degree of their glycaemic control. MATERIALS AND METHODS The study was conducted at the outpatient clinic of Internal Medicine department at Owaisi Hospital and Research Centre, Hyderabad. The study included 100 patients of clinically proven Type 2 Diabetes mellitus with HbA1c levels below or equal to 6.5% and 100 patients with HbA1c levels above 6.5%. Patients with associated co-morbid conditions like congestive cardiac failure, chronic renal failure, stroke, haematological disorders, malignancy, obstetric and gynecological disorders, patients on hormone therapy, patients on antiplatelet therapy, pregnancy were excluded from the study. Documentation of detailed history of present and past illness, treatment history, family history of all the participants of the study was done. Anthropometric measurements like Height, Weight and BMI were documented. Available data from recent haematological reports (within 1 week) of the cases was documented following which blood sample was collected under aseptic precautions, in EDTA vacuum evacuated tubes for Complete Haemogram and Peripheral Blood Picture and in Fluorides EDTA vacuum evacuated tubes for estimation of Blood Glucose by Glucose Oxidase Enzymatic Method and Glycosylated Hemoglobin by Ion Exchange Resin Method.The data collected were analyzed and expressed as Mean ± SD. Student’s unpaired t test was used to compare the data. Statistical software SPSS 22.0 was used for the analysis of the data and Microsoft Word and Excel to generate graphs and tables. Level of Significance: P < 0.05 was considered as significant while analyzing the data. RESULTS The present study included 200 Type 2 diabetes patients divided into two groups based on their glycaemic control ; Good glycaemic control diabetic group (HbA1c ≤ 6.5%) - Group A and poor glycaemic control diabetic group (HbA1c > 6.5%) - Group B. The mean age of diabetics in Group A was 51.14 ± 9.04 years and the mean age of diabetics in Group B was 50.01 ± 9.60 years (Table 1).
Table 1: Comparison of mean ages in the two groups
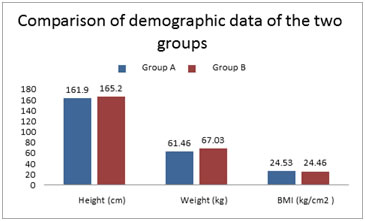
The overall female: male ratio was 68:32. The demographic variables of the two groups were documented and compared and showed no significant difference as shown in fig.1. Amongst the diabetics, a total of 45 of 100 (45%) gave a positive family history of diabetes while 55% had no family history of diabetics. The mean blood sugars and serum creatinine were estimated in the two groups. (Table 2) Table 2: FBS,PPBSand Serum creatinine in the two groups
Figure 1: Comparison of demographic data of the two groups
The overall mean platelet count was 218161± 4384 in Group A diabetics and 343500 ± 2905 in Group B diabetics (Table3). There was a statistically significant difference in platelet count of diabetics in Group A and those in Group B (p < 0.01).
Table 3: Mean Platelet count in relation to glycaemic control in the two groups
DISCUSSION The platelet counts are remote indicators of thrombotic potential, and risk factors for micro-vascular complications in diabetics 8-10. In the present study, the mean platelet count in the uncontrolled diabetic group was higher than that of the controlled diabetic group that was similar to the studies done by Demirtunc et al11 and Zuberi et al9. Other studies by Hekimsoy et al8 had observed the opposite findings of lower platelet count in diabetic subjects as compared to normal healthy subjects. Hence, the platelet count could be dependent on several variables, that is, mean platelet survival, platelet production rate and turnover rate in DM. However, increased platelet count may lead to increased platelet reactivity and platelet aggregation consequently leading to increased micro and macro-vascular complications. This aspect needs to be further studied in larger groups with better predictors of platelet aggregation like Mean platelet volume. Nevertheless the importance of adequate glycaemic control for optimum platelet function to decrease or delay progression of macro and micro-vascular complications in diabetes cannot be overemphasized. Platelet count and MPV might be used as a simple and cost-effective laboratory test in the follow up of diabetes mellitus along with HbA1c and thereby help to reduce the morbidity and mortality.
CONCLUSION Most of the patients with type 2 DM suffer from preventable vascular complications and early diagnosis of derangements in coagulation can help manage these vascular diseases successfully. Therefore, Platelet count, MPV and HbA1c can be a useful as prognostic marker of cardiovascular complication in diabetics. Thus it is recommended that treatment criteria for diabetes should include routine hematological tests and take into consideration the inevitable consequences of aging, and poor glycaemic control, in order to make optimal therapeutic decisions for the prevention of complications of diabetes mellitus in adults.
REFERENCES
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.