|
Table of Content Volume 10 Issue 2 - May 2019
A study of pre-treatment characteristics and depressive symptoms in patients of first episode of psychosis
Nitin P Patil1, Samir V Gupte2*, Sudhir J Gaikwad3, Sachin U Ghatge4, Sagar V Kulkarni5
Mahesh A Kumbhar6
1,2Associate Professor,3,4,5,6Assistant Professor, Department of Psychiatry, Bharati Vidyapeeth (Deemed To be University) Medical College And Hospital, Sangli, Maharashtra-416 414, INDIA.
Email: drnitinpatil@gmail.com , samirguptegnh@yahoo.co.in
Abstract Background: Depressive symptoms are commonly observed in first episode psychosis. Course of depression affects the prognosis and treatment of psychosis. Aim and objective: To study the pre treatment characteristics and depressive symptoms in patients of first episode of psychosis Methodology: Present study carried out in 200 patients diagnosed as first episode psychosis at a tertiary health care centre. Data was collected with pre tested questionnaire. Data included sociodemographic characterstics, detailed history and clinical examination. Diagnosis was done by principal investigator according to ICD 10 –Classification of Mental Behavioral Disorder Diagnostic Criteria. For Schizophrenia, schizotypal and delusional disorders F20-F29 and Mood (affective) disorders F30-F39. Assessment scales used in Current study were PANSS scale, CDSS, GAF etc. patients were followed after 12 months and assessed with these scales again. Data was analysed with appropriate statistical tests. Results and discussion: Mean age of the patients was 31.26± 4.32 years. 0ut of total 200 patients 78% were male and 22 % were females. Out of total 200 patients 93 (46.5%) have CDSS score of 6 or more at baseline. At follow up after one year 65 (33.5%) patients had score of 6 or more. Among the sociodemographic variables gender shows significant correlation with baseline CDSS scores. Duration of untreated psychosis, GAF symptoms, GAF Function, PNASS depressive and PNASS total. shows correlation at baseline as well as at follow up. (0.23 and 0.30)
Key Word: depressive symptoms.
INTRODUCTION
Epidemiology of first episode psychosis is poorly understood because of various reasons. The concept of first episode psychosis is varied from one episode to another. Some of the studies have included Schizophrenia and Schizophrenia spectrum disorders only. While others have included Affective Disorders with or without psychotic features, i.e. Major depressive disorder and Manic episodes. Some of the studies have included Substance induced psychotic disorders and Substance use as a morbidity. Age limit is arbitrarily fixed between 18 to 64 years. Even though in many cases onset of Schizophrenia and Affective disorder is in adolescent age, before 18 years, Occurrence of first episode psychosis in elderly above age of 65years. Patients of first episode psychosis may not come in contact with health care services as soon as initial symptoms develop due to various reasons. Inadequate number of Psychiatrists and paramedical professionals, their uneven distribution in society, lack of awareness about mental disoders, and its scientific treatment, to name some of them. Depression is commonly observed in patients of first episode psychosis. 1-4Depressive symptoms occur in different phases of the psychosis, mainly prodromal, acute and post-psychotic phases 5-9. This study aimed at finding of pretreatment characterstics and depressive symptoms in patients of first episode psychosis.
AIM AND OBJECTIVE
To study the pre treatment characteristics and depressive symptoms in patients of first episode of psychosis
MATERIAL AND METHODS
Present study carried out in 200 patients with first episode of psychosis at a tertiary health care centre. All patients attending psychiatry OPD and diagnosed as first episode psychosis were studied.
INCLUSION CRITERIA
- Patients diagnosed with first episode psychosis (Schizophrenia ,schizotypal and delusional disorders and Mood disorders)
- Patients above 12 years of age
EXCLUSION CRITERIA
- Patients below 12 years
- Patients not willing to participate in the study
- Patients suffering from organic brain syndromes, dementia, delirium ,mental retardation, substance induced psychotic disorders, withdrawal states and intoxication of various chemicals, dissociative disorders, malingering and neurological disorders
Study was approved by ethical committee. A valid written consent was taken from the patient or caregiver after explaining study to them. Data was collected with pre tested questionnaire. Data included sociodemographic characterstics such as age, sex. Detailed history of the patient was taken. Pretreatment characterstics of the patient were noted. Through clinical examination was done by the principal investigator. Diagnosis was done by principal investigator according to ICD 10-Classification of Mental Behavioral Disorder Diagnostic Criteria For Schizophrenia, schizotypal and delusional disorders F20-F29 and Mood (affective ) disorders F30-F39.10 Assessment scales used in Current study were PANSS scale, CDSS, GAF etc. symptom severity was assessed by the Positive and Negative Syndrome Scale (PANSS)11 This scale is characterized by five subscales; positive, negative, excitative, depressive, and cognitive 12. Depression was assessed using the Calgary Depression Scale for Schizophrenia (CDSS)13. In our study we took cut off point of ≥6 in line with the previous studies14,15. General level of symptoms and functioning was assessed with the Global Assessment of Functioning scale (GAF), split version16,17 patients were followed after 12 months and assessed with these scales again. CDSS compared at baseline and follow up after 12 months. Data was analysed with appropriate statistical tests.
RESULTS
Total 200 patients were studied. Mean age of the patients was 31.26± 4.32 years. 0ut of total 200 patients 78% were male and 22 % were females. Marital status was assessed as married, divorced and unmarried. 0ut of 200 patients 140 (70%) were married, 11% were divorced/ widow and 19% were unmarried. Table 1 shows other sociodemographic characterstics. Mean years of education were 10.2±2.73 years. Mean DUP (duration of untreated psychosis) was 46.3± 4 .9 weeks. Among all 69 % patients had history of traumatic life event. past history of suicide attempt was observed in 14% population. Clinical condition of the patients was assessed by PANNS score. Mean values of PANNS score was given in table 1. Figure 1 shows distribution of patients according to diagnosis. Schizophrenia is most commonly (53%) observed. Schizoaffective disorders were seen in 5% population. Schizophreniform disorders were seen in 9% patients. delusional disorders (5.5%), brief psychiatric disorders (4%), psychotic disorders (4%) and others were 19.5%. Out of total 200 patients 93 (46.5%) have CDSS score of 6 or more at baseline. At follow up after one year 65 (33.5%) patients had score of 6 or more. The association between characteristics of these patients and CDSS score at baseline and follow up are shown in table 2. Among the sociodemographic variables gender shows significant correlation with baseline CDSS scores. Age and years of education did not show any correlation at baseline as well as at follow up. Duration of untreated psychosis shows correlation at baseline as well as at follow up. (0.23 and 0.30) At baseline GAF symptoms, PANNS excitative, PNASS depressive and PNASS total showed significant correlation. At follow up CDSS scores were significantly correlated with GAF symptoms, GAF Function, PNASS depressive and PNASS total.
Table 1: Baseline characteristics of patients of first episode psychosis
Sr no |
Characteristics |
Mean |
Standard deviation |
1 |
Age (years) |
31.26 |
4.32 |
2 |
Years of education (years) |
10.2 |
2.73 |
3 |
DUP (weeks) |
46.3 |
4.9 |
4 |
PANNS positive score |
14.78 |
4.2 |
5 |
PANNS negative score |
20.01 |
5.11 |
6 |
PANNS excitative score |
9.23 |
2.38 |
7 |
PANNS depressive score |
13.72 |
3.21 |
8 |
PANNS general score |
36.3 |
8.1 |
9 |
PANNS total score |
71.42 |
15.4 |
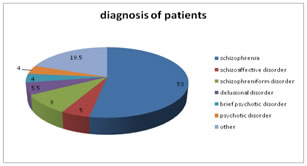
Figure 1: Distribution of patients according to diagnosis
Table 2: Sociodemographic and clinical characteristics in patients of first episode of psychosis and their correlates with CDSS score at baseline and follow up.
Sr no |
Characteristics |
Mean (SD) |
Correlation with
Baseline CDSS score |
Correlation with
Follow up CDSS score |
1 |
Age |
31.26(4.32) |
0.01 |
0.1 |
2 |
Gender (male ) (156) |
|
0.17* |
0.11 |
3 |
Education in years |
10.2 (2.73) |
-0.03 |
-0.1 |
4 |
DUP |
46.3 (4.9) |
0.23** |
0.30** |
|
PANSS SCORE |
5 |
PANSS positive |
14.78 (4.2) |
0.06 |
0.05 |
6 |
PANSS negative |
20.01(5.11) |
0.11 |
0.19 |
7 |
PANSS excitative |
9.23(2.38) |
0.22* |
-0.04 |
8 |
PANSS depressive |
13.72(3.21) |
0.57** |
0.36** |
9 |
PANSS total |
71.42 (15.4) |
0.28** |
0.22** |
|
GAF score |
10 |
GAF symptoms |
40.35(10.4) |
-0.28** |
-0.27** |
11 |
GAF function |
43.21(11.7) |
-0.12 |
-0.23* |
*significance at level 0.05 ** significance at level 0.01
DISCUSSION
Total 200 patients were studied. Mean age of the patients was 31.26± 4.32 years. Out of total 200 patients 93 (46.5%) have CDSS score of 6 or more at baseline. At follow up after one year 65 (33.5%) patients had score of 6 or more. Similarly depressive symptoms decreased after follow up in previous studies.18-21. Among the sociodemographic variables gender shows significant correlation with baseline CDSS scores. Age and years of education did not show any correlation at baseline as well as at follow up. Duration of untreated psychosis shows correlation at baseline as well as at follow up. (0.23 and 0.30) At baseline GAF symptoms, PANNS excitative, PNASS depressive and PNASS total showed significant correlation. At follow up CDSS scores were significantly correlated with GAF symptoms, GAF Function, PNASS depressive and PNASS total. Previous studies showed different results. Bottlender et al3 found that depressive symptoms in the acute psychotic phase was a positive prognostic indicator for patients concerning negative symptoms. Riedel et al found that depressed first-episode schizophrenia patients scored significantly higher on all PANSS subscales. 20 Cotton et al 19 studied differences in the clinical and functional characteristics of FEP patients with and without depressive symptoms. The group with depressive symptoms at baseline was less hospitalized and had less substance abuse during treatment. At discharge patients in this group had better insight concerning their illness. The depressed group of patients showed past diagnosis of personality disorder, suicide attempts, ongoing substance abuse, lower GAF mean score. Upthegrove et al 21 studied the course of depression in prodromal, acute, and 12 months follow-up period of psychosis among 82 patients. They found that Severity of depression was not significantly correlated with the severity of positive and negative symptoms in the acute or follow-up phases. Oosthuizen et al22 followed the patients for 2 years. They observed that depressive symptoms in acute psychotic phase were different from post psychotic period. Depressive symptoms in acute period improved after antipsychotic treatment but symptoms in post psychotic period did not resolved after antipsychotic ttreatment alone. These were referred as ‘persistent depressive symptoms’.
CONCLUSION
Depressive symptoms are common in first episode psychosis both at baseline and 12 months follow up. CDSS score decreased at 12 months follow up. Gender, duration of untreated psychosis and PNASS score correlated with CDSS at base line and follow up. These factors are helpful for management and prognosis of psychosis.
REFERENCES
- Sim K, Mahendran R, Siris SG, Heckers S, Chong SA: Subjective quality of life in first episode schizophrenia spectrum disorders with comorbid depression. Psychiatry Res 2004, 129:141–147.
- Addington D, Addington J, Patten S: Depression in people with firstepisode schizophrenia. Br J Psychiatry Suppl 1998, 172:90–92.
- Bottlender R, Strauss A, Moller HJ: Prevalence and background factors of depression in first admitted schizophrenic patients. Acta Psychiatr Scand 2000, 101:153–160.
- Romm KL, Rossberg JI, Berg AO, Barrett EA, Faerden A, Agartz I, et al: Depression and depressive symptoms in first episode psychosis. J Nerv Ment Dis 2010, 198:67–71.
- Salokangas RK, Mc Glashan TH: Early detection and intervention of psychosis. A review. Nord J Psychiatry 2008, 62:92–105.
- Hafner H, Maurer K, Trendler G, An Der Heiden W, Schmidt M: The early course of schizophrenia and depression*. Eur Arch Psychiatry Clin Neurosci 2005, 255:167–173.
- Levy ST, Mc Glashan TH, Carpenter WT Jr: Integration and sealing-over as recovery styles from acute psychosis. J Nerv Ment Dis 1975, 161:307–312.
- Knights A, Hirsch SR: “Revealed” Depression and drug treatment for schizophrenia. Arch Gen Psychiatry 1981, 38:806–811.
- Birchwood M, Iqbal Z, Upthegrove R: Psychological pathways to depression in schizophrenia: studies in acute psychosis, post psychotic depression and auditory hallucinations. Eur Arch Psychiatry Clin Neurosci 2005, 255:202–212.
- World Health Organisation. (1992). The ICD-10 Classification of Mental and Behavioural Disorders: Clinical Descriptions and Diagnostic Guidelines. Geneva: World Health Organisation.
- Kay SR, Fiszbein A, Opler LA: The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr Bull 1987, 13:261–276
- Bentsen H, Munkvold OG, Notland TH, Boye B, Bjorge H, Lersbryggen AB, et al: The interrater reliability of the positive and negative syndrome scale (PANSS. In Int J Methods Psychiatr Res 1996, 3:227–235.
- Addington D, Addington J, Schissel B: A depression rating scale for schizophrenics. Schizophr Res 1990, 3:247–251.
- Martin-Reyes M, Mendoza R, Dominguez M, Caballero A, Bravo TM, Diaz T, et al: Depressive symptoms evaluated by the calgary depression scale for schizophrenia (CDSS): genetic vulnerability and sex effects. Psychiatry Res 2011, 189(1):55–61.
- Schennach-Wolff R, Obermeier M, Seemuller F, Jager M, Messer T, Laux G, et al: Evaluating depressive symptoms and their impact on outcome in schizophrenia applying the calgary depression scale. Acta Psychiatr Scand 2011, 123(3):228–238.
- Jones SH, Thornicroft G, Coffey M, Dunn G: A brief mental health outcome scale-reliability and validity of the global assessment of functioning (GAF). Br J Psychiatry 1995, 166:654–659.
- Pedersen G, Hagtvet KA, Karterud S: Generalizability studies of the global assessment of functioning-split version. Compr Psychiatry 2007, 48:88–94.
- Knights A, Hirsch SR: “Revealed” Depression and drug treatment for schizophrenia. Arch Gen Psychiatry 1981, 38:806–811.
- Cotton SM, Lambert M, Schimmelmann BG, Mackinnon A, Gleeson JF, Berk M, et al: Depressive symptoms in first episode schizophrenia spectrum disorder. Schizophr Res 2012, 134:20–26.
- Riedel M, Mayr A, Seemuller F, Maier W, Klingberg S, Heuser I, et al: Depressive symptoms and their association with acute treatment outcome in first-episode schizophrenia patients: comparing treatment with risperidone and haloperidol. World J Biol Psychiatry 2012, 13:30–38.
- Upthegrove R, Birchwood M, Ross K, Brunett K, McCollum R, Jones L: The evolution of depression and suicidality in first episode psychosis. Acta Psychiatr Scand 2010, 122:211–218.
- Oosthuizen P, Emsley R, Niehaus D, Koen L, Chiliza B: The relationships between depression and remission in first-episode psychosis. World Psychiatry 2006, 5:172–176.
|
|
 Home
Home This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.