 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content Volume 10 Issue 3 - June 2019
A study on correlation of lithium and renal dysfunction with estimated glomerular filtration rate
Syed Ummar Ibrahim1, Fathima Nasreen Jaffar Hussain2, Jayachandran G3, Sureshkumar Ramasamy4*
{1Associate Professor, 4Assistant Professor, Department of Psychiatry} {2Junior Resident, 3Professor & HOD, Department of Biochemistry} PSG IMS & R, Coimbatore. Tamil Nadu, INDIA. Email: docsureshkumar2012@gmail.com , drsureshkumar99@gmail.com
Abstract Objectives: Lithium has been used in the treatment of mood disorders but its use is limited for its narrow therapeutic window and renal dys function. We aimed to correlate severity of renal dysfunction with duration of lithium therapy and serum lithium levels. We also analysed patients with Lithium induced renal dysfunction with normal creatinine values, but with abnormal eGFR. Methods: We included Bipolar patients who are on atleast2 years of Lithium therapy & with minimum of 2 serum Creatinine values during treatment, baseline & 6months post-baseline. We recruited 906patients, only 55 patients qualified for our inclusion criteria. We had 110 creatinine values & we calculatedeGFR based on Modificationof Diet in Renal Disease study group formula. We correlated duration of lithium therapy, serum lithium levels with average S.Creatinine levels and average eGFR. Results: There was no correlation between duration of lithium treatment with average serum creatinine values ( r = -0.17 ) or average eGFR ( r = +0.24).There was no correlation between serum lithium levels with average serum creatinine values ( r = -0.04) and average eGFR ( r = -0.06 ).Among 19 patients with high serum creatinine values , almost all except one had Grade 2 renal dysfunction eGFR value Conclusion: Neither the duration of lithium therapy (upto 17 years) , nor serum lithium levels correlated with renal dysfunction. Fifteen percent of patients with normal creatinine levels had early renal dysfunction on eGFR, indicating probably eGFR as anearly indicator than creatinine. Key Word: fLithium, Creatinine, Renal dysfunction, eGFR, Estimated Glomerular filtration rate
INTRODUCTION Lithium has been used in the treatment of mood disorders for several decades. But its use is limited for its narrow therapeutic window and multiple systemic side effects.Various studies were done to find the relationship between the serum lithium levels, duration of therapy, and dosage of lithium carbonate with its clinical responses. Among the available psychotrophics, Lithium remains a key drug especially in maintenance therapy. Lithium needs regular monitoring of serum lithium levels and renal dysfunction because of its narrow therapeutic window, as it is excreted nearly exclusively through the kidneys. The effect on Lithium induced renal dysfunction remains a controversy for more than four decades. Histopathological changes have been demonstrated way back in 1977, concluding chronic renal disease may develop only in patients with renal concentration of lithium reaches toxic level- either periodically or continuously.1 The duration of lithium treatment and cumulative dose has been suggested as major determinants of nephrotoxicity, but were only from small case series with multiple methodological issues.2,3 Previous meta- analysis have shown poor quality, emphasizing the need for large scale studies. 4,5 In the study by Stephen Clos et al, no effect was found on rate of eGFR change over time in euthymic BPAD patients on Lithuim maintenance therapy.6Lithium causes a modest decline in renal function. However, the available research suggests that ESRD is a very rare complication of long-term lithium treatment, affecting ∼1% of patients who have taken lithium for over 15 years.7With this above background, we planned for a study aiming for correlation of severity of renal dysfunction with duration of lithium therapy and serum lithium levels. We also did a correlation between socio-demographic variable and severity of renal dysfunction. We also analysed patients with Lithium induced renal dysfunction with normal creatinine values, but with abnormal eGFR. METHODS We included patients with bipolar affective disorder who are on atleast2 years of Lithium therapy & with minimum of 2 serum Creatinine values during the treatment, one at baseline & atleast one after>= 6 months post-baseline. We excluded patients who were on short duration of lithuim treatment (< 2 years) or who had only one/no serum creatinine value. We also excluded patients who were on not on follow-up at PSG. We retrieved 1296 Serum lithium values of Bipolar affective disorder patients from PSG Hospitals MRD records (2013 – 2017). 522 values were repeat serum lithium values of same patient. Hence 774 patients with all the available lithium values were included. 295 patients excluded , as they were all inpatients and they had another out-patient file. Among the remaining 499 patients, 339 patients were excluded (160 patients were left), as they had one or no serum creatinine value.105 patients were excluded as they did not have serum creatinine values both at baseline and 6months post-baseline. Finally, 55 Patients were analysed for the study. We had 121 creatinine values & we calculated corresponding eGFR based on Modificationof Diet in Renal Disease (MDRD ) study group formula,8eGFR (mL × min–1× [1.73 m2] -1 )= 175 × (S Cr standardized [mg × dL–1]) –1.154× (age [years ] )–0.203Correction factor: for women × 0.742 for blacks × 1.18 186 x [Plasma Creatinine (μmol/L) x 0.0011312] -1.154 x[age (years)] -0.203x [0.742 if female] x [1.212 if black] The following categories of eGFR were considered, as per KDOQI criteria. 9 Grade 1 -> 90 ml/min/1.73 m2: Grade 2 – 60 to 89 ml/min/1.73 m2: Grade 3a – 45 to 59 ml/min/1.73 m2: Grade 3b–30 to 44 ml/min/1.73 m2: Grade 4– 15 to 29 ml/min/1.73 m2 : Grade 5–<15 ml/min/1.73 m2.We analyzed baseline socio-demographic variables , namely, age & sex .We categorized age into adolescence, adults & geriatric population. We also analysed the co-morbidities, duration of follow-up after initiation of study, serum Lithium Level, total serum Creatinine values & total eGFR values. We correlated duration of lithium therapy with patients average S.Creatinine levels and average eGFR. We also correlated serum lithium levels with patients average S.Creatinine levels and average eGFR. We compared patient’s serum creatinine level and the corresponding eGFR. We analysed patients having normal serum creatinine (<=1 mg/dl) values with patients having abnormal eGFR. Statistical Analysis: We analysed duration of lithium therapy, serum lithium levels, average serum creatinine levels , eGFR as a continuous measures. We used Pearsons correlation co-efficient to correlate duration of lithium therapy, serum lithium levels with serum creatinine and eGFR. If the r value is +1, it means a positive correlation and if it is1, it means a negative correlation. We also tabulated normal serum creatinine (<=1 mg/dl) values withabnormal eGFR in varying ranges.
RESULTS Majority of the patients were men & in adult age group. Majority of patients followed upto 5 years & more than two-fifth followed up more than 5 years. Diabetes was the commonest co-morbidity. Six percentage of patients had serum lithium level in toxic range. Seventeen percentage of patients had serum creatinine value more than one. Thirty percentage of patients had eGFR less than 90.
Table 1: Socio-demographic variables at baseline and Lithium parameters
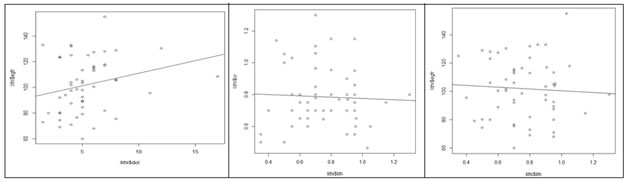
Figure 1 Figure 2 Figure 3 Figure 1: Pearsons Correlationcurve comparing duration of Lithium therapy with average serum creatinine values: Figure 2: Pearsons Correlation curve comparingserum lithium levels with average serum creatinine values; Figure 3: Pearsons Correlation curve comparingserum lithium levels with average estimated Glomerular filtration rate Figure 1, The above curve denotes no correlation between duration of lithium treatment with average eGFR (r =+0.24). Figure 2, The above curve denotes no correlation between serum lithium levels with average serum creatinine level (r = -0.04). Figure 3, The above curve denotes no correlation between serum lithium levels with average eGFR ( r = -0.06 ).
Table 2: Comparison of patients with normal creatinine levels with low eGFR
Among 102 (102 / 121) normal serum creatinine values, 15 serum creatinine values (14.7 %) had low corresponding eGFR values. Table 3: Comparison of patients with high creatinine levels with eGFR values.
All the patients, except one had Grade 1 renal dysfunction, eGFR between 60 to 98.
DISCUSSION We did a retrospective study on effect of lithium levels and duration of lithium therapy on renal dysfunction.Majority of the recruited were adult men with diabetes as the common co-morbidity. The duration of lithium therapy, did not correlate with renal dysfunction in-terms of serum creatinine values. Three patients were on treatment for more than ten years, one for even seventeen years. The corresponding eGFR values also did not correlate with duration of lithium therapy. Previous studies and meta-analysis also concluded the same result. In the study by Stefan Clos et al, both, duration of exposure to lithium and mean serum lithium level were not significant predictors for eGFR decline.Our study also reveals serum lithium level (which is a marker of adequacy of lithium dose), did not correlate with renal dysfunction, either by creatinine levels or eGFR levels. Previous studies have shown that exposure to lithium (in the absence of episodes of toxicity) is a causal factor and the length of lithium exposure as a predictor of renal dysfunction.10,11 In contrary, our study did not show correlation. A large UK community sample study by Miney et al12 had a short observation period of 2 years and did not analyse longitudinal changes. In our study patients were on lithium, even for 17 years and the mean duration of lithium was five years. In a UK cohort study, Close and colleagues 13 used diagnostic codes for adverse renal outcomes rather than eGFR. We preferred eGFR as an indicator of renal dysfunction as it is a better predictor than serum creatinine. In an observational study by, Aprahamian and colleagues,14 a single-blind follow-up study , no significant change in renal function of elderly patients after 4 years of chronic low-dose lithium use , as evidenced by our study. About fifteen patients (15 %), with normal creatinine levels had low eGFR values, indicating eGFR could pick-up renal dysfunction early. Among 19 patients with high serum creatinine values, almost all except one had Grade 2 renal dysfunction eGFR value .A single patient had grade 3 renal dysfunction 9 ( eGFR –57 ).Our study limitations are , retrospective study design which has its own critics. The sample size was small and hence results can’t be generalized. Mean duration on lithium was five years; a longer study would be of more credit. We could have had a control population, with which we would have analyzed in a better way. Our study was an observational study , hence only the available creatinine & lithium level were used for analysis.Almost one-third of patients had a co-morbid physical illness , disorders like diabetes and hypertension is known to cause renal dysfunction. Cockcroft-Gault equation is well suited for estimation of GFR changes during pharmacotherapy, instead we used MDRD equation, which is applied in adults with chronic renal disease.The National Kidney Foundationgrades chronic kidney disease based on kidney damage ( for ≥ 3 months, as defined by structural of functional abnormalities of the kidney, with or without decreased GFR, manifest by either : Pathological abnormalities; or markers of kidney damage, including abnormalities in the composition of the blood or urine, or abnormalities in imaging tests) and eGFR. In our study, we used only eGFR as an indicator of renal dysfunction. The strengths of our study are, we had a strict inclusion criteria, thereby excluded patients an acute phase of lithium treatment (less than two years of treatment). We included patients only with post-baseline creatinine levels, atleast after 6 months, hence had a minimum renal exposure to lithium.
CONCLUSION In our study, neither the dosage (analysed with serum lithium level), nor the duration of lithium treatment, caused renal dysfunction. Hence, clinicians prescribing lithium need not be anxious on renal parameters, but need to monitor as per guidelines. We would also recommend clinicians to monitor eGFR than creatinine, to identify renal dysfunction early.
REFERENCES
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.