|
Table of Content Volume 10 Issue 3 - June 2019
A prospective study of stability of diagnosis and adherence to treatment in patients of first episode psychosis
Nitin P Patil1, Samir V Gupte2*, Sudhir J Gaikwad3, Sachin U Ghatge4, Sagar V Kulkarni5
Mahesh A Kumbhar6
1,2Associate Professor,3,4,5,6Assistant Professor, Department of Psychiatry, Bharati Vidyapeeth (Deemed To be University) Medical College and Hospital, Sangli, Maharashtra-416 414, INDIA.
Email: drnitinpatil@gmail.com , samirguptegnh@yahoo.co.in
Abstract Background: Psychosis contributes major part in psychiatric diseases. Diagnostic stability is important for treatment guidelines in psychosis. Treatment adherence plays an important part in prognosis of first episode psychosis. Aim and objective: to study the stability of diagnosis and adherence to treatment in patients of first episode psychosis. Material and methods: Present study carried out in 200 patients with first episode of psychosis at a tertiary health care centre. Diagnosis was done by principal investigator according to ICD 10-Classification of Mental Behavioral Disorder Diagnostic Criteria They were treated according to diagnosis and guidelines for the treatment. Patients were followed up at one year. Adherence to treatment checked. Data analysed with appropriate statistical tests. Results: Mean age of the patients was 31.26± 4.32 years. In our study stability of diagnosis was higher for schizophrenia and schizoaffective disorders. (65.84% and 70%, 6.21% and 8%). It was low for schizophreni from disorders (11.18% and 8%). It was intermediate for delusional disorders (6.83% and 5.33%) and psychotic disorders (9.94% and 8.67%). In our study regular adherence to the treatment was observed in 123 (65.08%) patients.
Key Word: psychosis.
INTRODUCTION
Psychotic symptoms typically include changes in thinking, mood and behavior. Symptoms vary from person to person and may change over time. According to study by Wiersma et al, 59% continue to experience moderate to severe social disability even after 15 years1 The two important sets of diagnostic criteria, the Diagnostic and Statistical Manual of Mental Disorders, 4th Edition (American Psychiatric Association, 2000)2 and the International Classification of Diseases, 10th Revision (World Health Organisation, 1992)3 are commonly used for diagnosis of first episode psychosis. studies found a greater stability for some first episode psychosis diagnoses as assigned using ICD-10 rather than DSM-IV criteria in the same patients,4while others found that both have equal consistency.5 Diagnostic stability is important to patients, doctors and caretakers. It provides general guidance for clinical decision making. Stability is important for development of treatment guidelines. Several studies were done in past focusing on stability of diagnosis of first episode psychosis. They showed varied results. In some studies suggest schizoaffective disorder has the highest 2 years prospective diagnostic stability, followed by affective spectrum psychosis and schizophrenia. 4Some studies suggest schizophrenia exhibited the highest 2 years prospective diagnostic stability, and the schizoaffective disorder the lowest stability.6 Treatment adherence is important factor in prognosis of psychosis. Present study aimed to see the diagnostic stability and treatment adherence in patients of first episode psychosis.
AIM and OBJECTIVE
to study the stability of diagnosis and adherence to treatment in patients of first episode psychosis.
MATERIAL and METHODS
Present study was carried out in 200 patients diagnosed as first episode psychosis. Present study carried out in 200 patients with first episode of psychosis at a tertiary health care centre. All patients attending psychiatry OPD and diagnosed as first episode psychosis were studied.
Inclusion Criteria
- Patients diagnosed with first episode psychosis (Schizophrenia, schizotypal and delusional disorders and Mood disorders)
- Patients above 12 years of age
Exclusion Criteria
- Patients below 12 years
- Patients not willing to participate in the study
- Patients suffering from organic brain syndromes, dementia, delirium ,mental retardation, substance induced psychotic disorders, withdrawal states and intoxication of various chemicals, dissociative disorders, malingering and neurological disorders
Study was approved by ethical committee. A valid written consent was taken from the patient or caregiver after explaining study to them. Data was collected with pre tested questionnaire. Data included sociodemographic characterstics such as age, sex. Detailed history of the patient was taken. Patients were examined by principal investigator. Diagnosis was done by principal investigator according to ICD 10-Classification of Mental Behavioral Disorder Diagnostic Criteria For Schizophrenia, schizotypal and delusional disorders F20-F29 and Mood (affective) disorders F30-F39.3 They were treated according to diagnosis and guidelines for the treatment. Patients were treated with antipsychotic medication and Electroconvulsive therapy. Patients were put on maintenance antipsychotic medication as per the consensus of the department of Psychiatry, They were followed up at one year. Again at these follow ups patients were clinically examined by the same investigator. Adherence to treatment checked. All data regarding diagnosis at follow up collected. Data analysed with appropriate statistical tests.
RESULTS
Total 200 patients were studied. Mean age of the patients was 31.26± 4.32 years. 0ut of total 200 patients 78% were male and 22 % were females. 0ut of 200 patients 140 (70%) were married, 11 % were divorced/ widow and 19% were unmarried. Mean years of education were 10.2±2.73 years. Mean DUP (duration of untreated psychosis) was 46.3± 4 .9 weeks. Figure 1 shows distribution of patients according to diagnosis. Schizophrenia is most commonly (53%) observed. Schizoaffective disorders were seen in 5% population. Schizophreniform disorders were seen in 9% patients. Delusional disorders (5.5%), brief psychiatric disorders (4%), psychotic disorders (4%) and others were 19.5%. Table 2 shows diagnosis stability in patients of first episode psychosis. Out of total 200 patients 39 patients were having psychosis related to general clinical conditions so those were not considered for diagnosis stability. Thus 161 patients were considered for baseline diagnosis. Majority of the patients at baseline were diagnosed as schizophrenia (65.84%). At the end of one year 11 patients were lost to follow up so only 150 patients were present at diagnosis of one year. It was observed from the table that stability of diagnosis was higher for schizophrenia and schizoaffective disordes. (65.84% and 70%, 6.21% and 8%). It was low for schizophrenifrom disorders (11.18% and 8%). It was intermediate for delusional disorders (6.83% and 5.33%) and psychotic disorders (9.94% and 8.67%). In our study out of total 200 patients 11 lost to follow up. Out of remaining 189 patients regular adherence to the treatment was observed in 123 (65.08%) patients. partial adherence was observed in 38 (20.11%) patients and non adherence was observed in 28 (14.81%) patients.
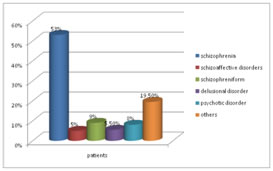
Figure 1: Distribution of patients according to baseline diagnosis
Table 2: stability of diagnosis in patients of first episode psychosis at baseline and one year follow up
Diagnosis |
Baseline diagnosis |
Diagnosis at one year |
|
No of patients |
Percentage |
No of patients |
Percentage |
Schizophrenia |
106 |
65.84% |
105 |
70% |
Schizoaffective disorders |
10 |
6.21% |
12 |
8% |
Schizophreniform |
18 |
11.18% |
12 |
8% |
Delusional disorders |
11 |
6.83% |
08 |
5.33% |
Psychotic disorders |
16 |
9.94% |
13 |
8.67% |
Total |
161 |
100 |
150 |
100 |
DISCUSSION
In our study Mean age of the patients was 31.26± 4.32 years. Similar findings were observed in Jager et al7 where they studied 73 patients of first episode psychosis and diagnosed them as per ICD 10 classification. Mean age of the patient in their study was 31.8 ± 14.6 years.310ut of total 200 patients 78% were male and 22 % were females. Similar findings were observed in previous studies where female patients ranged from 25% to 40%. 8-10 In our study Schizophrenia is most commonly (53%) observed. Schizoaffective disorders were seen in 5% population. Schizophreniform disorders were seen in 9% patients. Delusional disorders (5.5%), brief psychiatric disorders (4%), psychotic disorders (4%) and others were 19.5%. In our study stability of diagnosis was higher for schizophrenia and schizoaffective disordes. (65.84% and 70%, 6.21% and 8%). It was low for schizophrenifrom disorders (11.18% and 8%). It was intermediate for delusional disorders (6.83% and 5.33%) and psychotic disorders (9.94% and 8.67%). Similar results were seen in previous studies 11-13 In our study regular adherence to the treatment was observed in 123 (65.08%) patients. partial adherence was observed in 38 (20.11%) patients and nonadherence was observed in 28 (14.81%) patients. Similar findings were seen in Tan C et al14 where regular adherence was seen in 65.5% inividuals and non adherence was seen in 15% individuals.
CONCLUSION
In conclusion it can be said that about half of the patients diagnosed as first episode psychosis have fulfilled the diagnostic criteria of schizophrenia till the end of one year. Around one third of patients diagnosed as first episode psychosis remained regular adherent for one year.
REFERENCES
- Wiersma, D., Wanderling, J., Dragomirecka, E., Ganev, K., Harrison, G., An Der Heiden, W., Walsh, D. (2000). Social disability in schizophrenia: Its development and prediction over 15 years in incidence cohorts in six European centres. Psychological Medicine, 30, 1155-1167
- Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, 1994 (DSM-IV)
- World Health Organisation. (1992). The ICD-10 Classification of Mental and Behavioural Disorders: Clinical Descriptions and Diagnostic Guidelines. Geneva: World Health Organisation.
- Salvatore P, Baldessarini RJ, Tohen M, et al. McLeanHarvard International First-Episode Project: two-year stability of ICD-10 diagnoses in 500 first-episode psychotic disorder patients. J Clin Psychiatry. 2011; 72: 183–193.
- Heslin M, Lomas B, Lappin JM, et al. Diagnostic change 10 years after a first episode of psychosis. Psychol Med. 2015; 45: 2757–2769.
- Schwartz JE, Fennig S, Tanenberg-Karant M, et al. Congruence of diagnoses 2 years after a first-admission diagnosis of psychosis. Arch Gen Psychiatry. 2000; 57: 593–600.
- Moller HJ, Jager M, Riedel M, Obermeier M, Strauss A, Bottlender R. The Munich 15-year follow-up study (MUFUSSAD) on first-hospitalized patients with schizophrenic or affective disorders: assessing courses, types and time stability of diagnostic classification. Eur Psychiatry. 2011; 26: 231–243.
- Rufino AC, Uchida RR, Vilela JA, Marques JM, Zuardi AW, Del-Ben CM. Stability of the diagnosis of first-episode psychosis made in an emergency setting. Gen Hosp Psychiatry. 2005; 27: 189–193.
- Fraguas D, de Castro MJ, Medina O, et al. Does diagnostic classification of early-onset psychosis change over follow-up? Child Psychiatry Hum Dev. 2008; 39: 137–145.
- Kingston T, Scully PJ, Browne DJ, et al. Diagnostic trajectory, interplay and convergence/divergence across all 12 DSM-IV psychotic diagnoses: 6-year follow-up of the CavanMonaghan First Episode Psychosis Study (CAMFEPS). Psychol Med. 2013; 43: 2523–2533.
- Haahr U1, Friis S, Larsen TK, Melle I, Johannessen JO, Opjordsmoen S, Simonsen E, Rund BR, Vaglum P, McGlashan T.First-episode psychosis: diagnostic stability over one and two years.Psychopathology. 2008; 41(5):322-9.
- Narayanaswamy JC, Shanmugam VH, Raveendranathan D, Viswanath B, Muralidharan K. Short-term diagnostic stability of acute psychosis: data from a tertiary care psychiatric center in South India. Indian J Psychol Med. 2012; 34: 176–178.
- Schwartz JE, Fennig S, Tanenberg-Karant M, et al. Congruence of diagnoses 2 years after a first-admission diagnosis of psychosis. Arch Gen Psychiatry. 2000;57:593–600
- Tan C, Abdin E, Liang W, Poon LY, Poon NY, Verma S. Medication adherence in first-episode psychosis patients in Singapore. Early Interv Psychiatry. 2018.
|
|
 Home
Home This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.