 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content Volume 10 Issue 3 - June 2019
A study of socio demographic profile of the patients with suicidal attempts referred by practitioner physicians in private setup
Hemant J Baxi
Assistant Professor, Department of Psychiatry, Government Medical College, Gondia, Maharashtra, INDIA. Email: hemantbaxi@gmail.com
Abstract Background: Suicide is the third leading cause of death among young adults worldwide. It not only causes Emotional burden but also Economic burden to Families. Objectives: To see Socio-Demographic profile of Suicide Attempter presenting to Psychiatry OPD referred from Private Practitioners. Material and Methods: This was Cross Sectional Study done on 50 Consecutive Cases of Suicide Attempters presenting to Psychiatry OPD. Informed Consent was taken. They were asked in detail about Socio-Demographic Profile and data was evaluated using Microsoft excel. Results: Out of total 50 cases, Males formed 23 (46%) while Females formed 27 (54%) of the study. Most common Age group for Males was found to be 26-35 which formed 39%, Hindu formed 94% of the study, Unmarried were 31 (62%), most 33 (66%) came from Nuclear families, only 6 (12%) were Graduated, most 28 (56%) were Unemployed, most 27 (54%) had Income below Rs 6000/-, 26 (52%) showed some kind of Substance Abuse, 31 (62%) belonged to Rural Locality. Conclusions: Socio-Demographic data can be useful to access the problems faced by Suicide Attempters to help them to motivate for a better life. Keywords: Suicide, Socio Demographic profile, Psychiatry.
INTRODUCTION Suicide is a world problem which takes about one million lives yearly.1Suicide is a complex, Multidimensional thing that has been studied from Philosophical, Sociological, and Clinical perspective since long now. Suicidal behavior and Suicidality can be arranged as a continuum ranging from Suicidal Ideation to Suicide Attempts and Deaths due to Suicide. Attempted Suicide is defined as a potentially Self-injurious act with a non serious outcome for which there is evidence, either explicit or implicit that the individual intended to end himself or herself. The action may or may not result in injuries.2 Out of every thousand individual who commit Suicide per day, 110 of these are said to be Indians.3Most of the Suicides (37.8%) in India are aged below 30 years of age. The fact that 71% of Suicides in India of person aged below 44 years imposes a huge Social, Emotional, and Economic burden on Nation.4 The recent phenomenon of “Cyber‑Suicide” in the internet Era is a further cause for worries;5-6 also due to the use of new ways of Suicide are associated with exponential increases in overall Suicide rates.7Traditionally, in Western literature Risks factors associated with Suicide, including Suicidal Attempts include Young Age (15‑24 years), Female Gender, Low Educational Attainment, Unemployment, Living Alone, and History of Socioeconomic Deprivation , Financial Issues, Rejection in Love affairs and Stressful Familial Relationships were the most common causes in our Country.8 In this regards, we tried to examine the Socio-Demographics of Suicide in our locality.
MATERIAL AND METHODS This study was a Cross Sectional study carried out in Private Hospital in 50 consecutive cases who were referred to Psychiatry OPD, this study was carried out for 1 year. For the convenience of this study we have taken 50 cases. The detailed history was taken at Psychiatry OPD referral within 1 week of Suicide Attempt after they were made stable by treatment. A preformed pretested Proforma was used for taking the history. Informed Consent was taken, all the doctor patients confidentiality was maintained. Data was entered in Microsoft Excel and Mean, Percentage was Calculated using Excel.
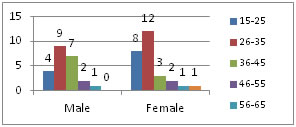
RESULTS Diagram 1: Age wise distribution of study population
Out of total 50 cases Males formed 23 (46%) while Females formed 27 (54%) of the study. Most common Age group for Males was found to be 26-35 which formed 39%, while 15-35 Age ranged formed 56% of the study, in Females age group of 16-35 formed 74% of the study.
Table 1: Sociodemographic profile of study population
Hindu formed 94% of the study, Unmarried were 31 (62%), most 33 (66%) came from Nuclear families, only 6 (12%) were Graduated, most 28 (56%) were Unemployed, most 27 (54%) had Income below Rs 6000/-, 26 (52%) showed some kind of Substance Abuse, 31 (62%) belonged to Rural locality. DISCUSSION This study was conducted to see the Socio-Demographic profile of Suicide Attempt cases coming to Psychiatry OPD. Out of total 50 cases Males formed 22 (44%) while Females formed 28 (56%) of the study, with Male :Female ratio of 1:1.27. The Mean Age was 27.2±7.6 SD. Most common Age group 9 (39%) for Males was found to be 26-35, while 15-35 age group formed 56% of the study. In Females, Age group of 16-35 formed 74% of the study. In Raja NS et al9 study, majority (25.5%) of the Study Subjects was in the Age group of 20–24 years, followed by 25–29 years and Male to Female ratio of 1.2:1. In Gade V et al10 study 30(41.6%) of the Patients were in the Age groups of 15-25 years. Nagendra MR et a11l concluded the peak Incidence of Suicidal Attempt between 15-29 years. This was in accordance with our study. Many Indian studies like Latha KS et al12, Elangbam V et al13 supported our findings. In Vishnu Gade Vet al10 study Male Patients were 38(52.8%) which were more than Females (47.2%). This dissimilarity was may be due Low Sample size and different Study location in our Study. Majority of case 94% belonged to Hindu religion which just signifies greater cases belonging to Hindu Religion, Religion and Suicide Attempt are not related. Similar was seen with Suresh Kumar PN et al14, Bharati S et al.15 In our study total married subjects were 38% while in a study done by Chandrasekaran R et al16it was 54%, in Lakshmi Swetha N et al17 study it was 60% this disparity was may be due to Larger sample size in their study. Low Education is said to be an Important Risk factor for Suicide across the World. Total number of illiteratesin this Study were 16% and Graduates were only 12%. In Chandrasekaran Ret al16 study illiteracy was 25% which was almost same as our results. Illiteracy was 42% and Graduates were 21% which was bit Higher than findings of our Study this may be because of different Socio Economic Status and Larger Sample in Gade V et al10 study. Total number of Unemployed in this study were 56%. Logaraj M et al18concluded that Unemployment was more Prevalent in Suicide Attempters this was in accordance with our Study. In this Study 53% cases belonged to Lowest Economic strata of the total cases. Agendra MR et al1l who also in accordance with our study said that most (83%) of the Suicidal Attempts were from the Low Socio-Economic groups. Majority of the case who Attempted Suicide were from Nuclear families. The more Responsibility of Family on Single person or Less Seniors to take care, coupled with Stress of modern life might have been responsible for huge larger number of cases similar was reported by Arun M et al.19 Substance Abuse was seen in 40% cases in Raja NS etal9while in this 52% cases showed Abuse of Some Substance. In this Study majority cases 62% belonged to Rural Areas, similar Rural Dominance 85% was reported by Gade V et al10 study. While Ramdurg S et al20 and Farooque et al21 who found more Suicide Attempts in urban areas.
CONCLUSION The Young Age Group represents the Most Vulnerable group in need. Low Education, Lower Economic Status, Unmarried Status, Nuclear Family, Unemployment, Rural locality and some sort of Substance Abuse was associated with Higher percentage of Suicidal Attempts in this study. Sooverall improvement in Employment, increased Education Status, Income sources, Strengthening of Family and Social values may decrease Suicidal Attempts. As this was a Cross Sectional study we cannot generalize this findings, more Sample size would have been better.
REFERENCES
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.