 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content Volume 12 Issue 2 - November 2019
The trend of anxiety symptoms during the different phases of the menstrual cycle in working women of reproductive age: An enquiry
Aneesh S Bhat1*, Tejal Gapchap2, Vaishali Korde3
{1Associate Professor, 2UG, Department of Psychiatry} {3Professor, Department of OBGY} MIMER Medical College, Talegaon Dabhde, Pune, Maharashtra, INDIA. Email:
Abstract Women in reproductive age group suffer from different emotional changes during the regular menstrual cycle. A lot of these emotional changes are severe enough to cause morbidity in functional, social, occupational life during the particular phase of menstrual cycle. A sound understanding about changes and trends of different emotions can be helpful to administer preventive strategies so as to improve the quality of life of women in reproductive age group. Many women experience Anxiety symptoms as a one of the major emotional symptoms during menstrual cycle. The study into trend of anxiety symptom will help to formulate the strategies to decrease these disturbances. The purpose of this study is to find the trend of anxiety in working women of reproductive age group. This study was carried out as a part of larger study. It is a prospective cohort study which included 124 participants. Participants were studied over three month period for different phases of menstrual cycle. Data were analysed using appropriate statistical method. Result obtained from this study shown that there is significant increase in anxiety in premenstrual and menstrual phase of the cycle. There is reduction in anxiety symptoms during ovulatory phase. Thus this study was successful in establishing increasing trend of anxiety symptoms towards late leuteal phase of cycle. These results were accordance with previous studies which has shown the similar trends of anxiety during different menstrual cycle . Key Words: Pre-Menstrual anxiety, Pre-Menstrual Dysphoric Disorder, Stress management, Anxiety, Becks anxiety inventory, working women.
INTRODUCTION Women of reproductive age group experience a number of symptoms like nervousness, sexual desire, insomnia, bloating, loss of appetite, irritability, etc. during particular phases of the menstrual cycle. Working women do experience more stress emotionally because of burden of responsibilities and difficulties in work life balance. The aim of study is to find out if there is any relationship between the specificity of the phase of menstrual cycle and the psychological disturbance like Anxiety that may occur during this phase. It was found that Somatic complaints such as abdominal pain and breast tenderness were significantly related to the luteal, premenstrual, and menstrual phases. Appetite increased in the peri-ovulatory and premenstrual phases. There was a tendency for sexual interest to be highest in the post-menstrual period. 1 The term Pre Menstrual Syndrome was introduced in the 1960s.2 Premenstrual syndrome (PMS) refers to physical and emotional symptoms that occur in the one to two weeks before a woman's period. Symptoms often vary between women and resolve around the start of menses. Its more severe form is called Pre Menstrual Dysphoric Disorder (PMDD).Currently it is estimated that 3-8% women of reproductive age meet strict criteria for PMDD. 13-18% women may have pre- menstrual dysphoric symptoms severe enough to induce impairment and distress. In this study, we wanted to find the trend of anxiety symptoms during different phases of menstrual cycle. PMDD is still under-recognised and needs to be brought into the eyes of the public. In the study 3, it was demonstrated that the burden of PMS/PMDD is in same magnitude as that of major recognised disorders. Hence, appropriate recognition of this disorder is necessary. Stress is almost always involved in PMS. Stress increases cortisol levels4, which blocks progesterone from its receptors, which sets the stage for estrogen dominance-causing symptoms like bloating, breast tenderness, mood swings, etc. in some women. Extra progesterone is necessary to overcome the blockade of its receptors by cortisol. When a woman discovers she has a handle on controlling her PMS, it will help her manage stress better. Then lower levels of progesterone will work normally again. Chronically elevated cortisol levels can be a direct cause of estrogen dominance, with all the familiar PMS symptoms. 5 Aim of this study is to find the severity and trend of psychological disturbance like Anxiety symptoms in females of reproductive age group during various phases of menstruation.
AIMS AND OBJECTIVES
MATERIAL and METHODS The subjects for the study were women in their reproductive age group which included students and staff from Professional Degree College. METHOD 1.A general information questionnaire was given at the enrolment for the study. 2.The participants were given General information questionnaire once, at the beginning of the study. There on, every following month (for 3 months), Becks Anxiety Inventory( BAI) was given to examine the anxiety symptoms during the 3 phases of the menstrual cycle. For this study, the menstrual cycle was divided into 3 phases- Day 6-12: Post Menstrual Stage Day 13-20: Ovulatory phase Day 21-28 + Day 1-5(menses): luteal or premenstrual phase + menstruation
The questionnaires were given as follows, to cover all phases of the cycle of a particular subject - 5th of 1st month- BAI+ Demographic Details 15th of 2nd month-BAI 25th of 3rd month-BAI The Anxiety scores were reflection of the severity of psychological distress, which are correlated to the phase of menstruation. TYPE OF THE STUDY Prospective cohort study. SAMPLE SIZE:– Calculated based on previous studies was 100-130 working women including staff and students of Professional College. SELECTION CRITERIA:A general information questionnaire were provided and then the suitable subjects were selected as per the inclusion and exclusion criteria after obtaining informed consent. INCLUSION CRITERIA: All women in reproductive age group with regular menses. EXCLUSION CRITERIA: 1.Women on hormonal contraceptives. 2.Post- menopausal women. 3. Pregnant women. 4. Women with pre-existing diagnosed psychological disorders and PCOD. RISK FACTORS: No risks are involved in this study. MATERIAL 1.General Information Questionnaire :- A Semi structured questionnaire to collect Socio Demographic information. 2.Becks Anxiety Inventory (BAI) This questionnaire was developed A.Beck et al This is 21 item questionnaire. This scale is a self-report measure of anxiety. Reliability: Internal consistency for the BAI = (Cronbach’s α=0.92) .Test-retest reliability (1 week) for the BAI = 0.75 (Beck, Epstein, Brown, and Steer, 1988). Validity: The BAI was moderately correlated with the revised Hamilton Anxiety Rating Scale (.51), and mildly correlated with the Hamilton Depression Rating Scale (.25) (Beck et al., 1988) Scoring:- The total score is calculated by finding the sum of the 21 items. Score of 0 = No Anxiety Score of 1– 21 = Mild anxiety Score of 22 – 35 = moderate anxiety Score of 36 and above =(severe) potentially concerning levels of anxiety STATISTICAL ANALYSIS:- Statistical analysis was done using appropriate software to calculate percentage of distribution of sample. RESULTS At the end of the study total n= 124 working women in reproductive age group participated in this study. Study carried out over three month’s period in different phases of menstrual cycle. At the end of study results were obtained by calculating the distribution and percentage of women belonging to each group of anxiety scale. Results are tabulated as shown in table 1.
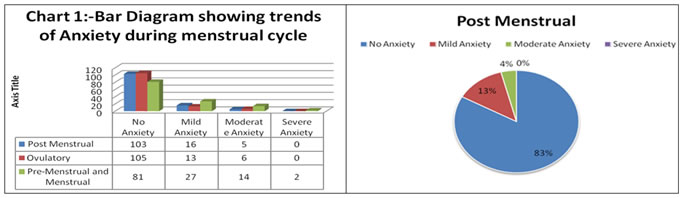
Table 1: Distribution of anxiety during different phases of menstrual cycle
From the above table and bar diagram following conclusion can be drawn. 1. Anxiety is one of the major symptoms during all three menstrual phases in females. 2. Anxiety symptoms had increased significantly during premenstrual and menstrual phases. 3. There is decline in anxiety which is noted in ovulatory phase of cycle. 4. In second phase of menstrual cycle anxiety symptom has shown incremental trend in all category of anxiety. 5. Increasing trend in anxiety shows the effect of hormonal changes in second phase of menstrual cycle on mood.
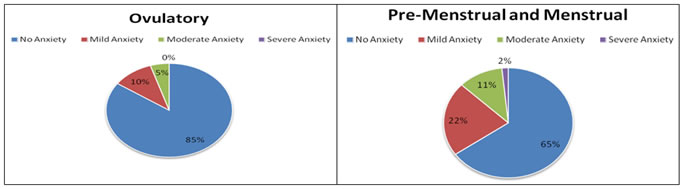
The following bar diagram shows clearly the distribution of anxiety in all phases of menstrual cycle. Chart 1 Chart 2 Chart 3 Chart 4 In chart 1, During post menstrual phase it is found that 83% females had no anxiety where as 13% has shown mild anxiety and 4% moderate anxiety,none had severe levelof anxiety symptoms; In chart 2, During Ovulatory phase 85% of females had no anxiety symptoms where as 10% had mild anxiety,5% had moderate anxiety,none shown severe anxiety. There was minor decrese in anxiety symptoms during ovulation; In chart 3, During Pre-Menstrual and Menstrual phase of cycle only 65% of females reported no anxiety symptoms which is less than previous phases where as 22% have shown mild anxiety ,11% had moderate anxiety, 2% had severe anxiety symptoms which is significantly greater than previous phases in which the percentage of females with anxiety symptoms was much lessor in each category; In chart 4, Thus results clearly indicates significant rise in anxiety symptoms during Pre-Menestrual and Menstrual phases of Menestrual cycle, which again advocate for attention to be paid for management of anxiety during this phase in females.
DISCUSSION The result of this study shows prevalence rate of anxiety including all severity to be around 35% in premenstrual phase, these results are in accordance with review of the PMDD literature by Kim and colleagues (2004) which reported that current comorbid prevalence rates among women with PMDD were 19–23% for Social Phobia and 4–38% for Generalized Anxiety Disorder. 8 In the current study it is seen that the anxiety symptoms were present in 15% females in Ovulatory phase and 17 % females in Post menstrual phase. In same group of females had shown higher anxiety symptoms during premenstrual phase which nearly doubled to 35% in this phase. These findings are similar to previous study which examined the symptom history of females with unexpected panic attacks .In this study 51% of women reported experiencing increased anxiety symptoms and 33% reported increased frequency of panic attacks premenstrually.9 In similar study 79% of women with Panic Disorder reported that they experienced an exacerbation of anxiety premenstrually.10 This suggests that the females who have premorbidly higher anxiety symptoms experience exacerbation in the anxiety during premenstrual and menstrual period. This indicates the trend of increasing anxiety towards third phase of menstrual period. The similar results are obtained from current study indicates the need to address this issue in females so as to prevent morbidity occurring during this phase because of excessive anxiety symptoms. Another study in which women with panic disorder who completed prospective daily diaries across two menstrual cycles, reported an exacerbation of anxiety and panic attacks during their premenstrual phase 11 A study in normal females reported increased anxiety in response to CO2 challenge during the premenstrual phase as compared to the postmenstrual phase1.12 Hormonal and neurobiological studies done in this regard indicates that Allopregnanolone or THP, a neuroactive metabolite of progesterone, rises and falls with progesterone levels during the menstrual cycle,with the sharpest rate of decline occurring during the premenstrual phase. THP is a potent positive modulator of GABA-A receptors, particularly at the δ and α4 subunits and rat models have consistently demonstrated that THP changes influence anxiety behavior. Especially a short-term exposure to THP has anxiolytic effects whereas rapid withdrawal which is experienced during the premenstrual phase induces particular subunit changes in the GABA-A receptor, which make it less effective and increases anxiety behaviors. 13,14.Thus neurochemically metabolite of progesterone THP is responsible for increase in anxiety symptoms in premenstrual phase.15 Another psychological investigation in this regard has reported that Women who reported higher emotion regulation difficulty experienced greater differences in perceived control over anxiety-related events between menstrual phases.16,17 Thus current study results are in accordance with previous studies done in females during all three phases of menstrual cycle .Thus from this discussion it can be concluded that there is a tendency of increase in anxiety symptoms towards premenstrual and menstrual phases. This is supported by neurochemical evidences also in previous studies. Strength of this study was in higher sample size compared to previous studies. The study is done over three months period prospectively; so data collected was more sensitive and has less confounding effect.
CONCLUSION AND LIMITATION From the result of this study it can be concluded that there is significant difference in anxiety symptoms during all three phases of menstrual cycle. Anxiety symptoms tend to increase towards premenstrual and menstrual phase of the menstrual cycle. Significant increase in anxiety in third phase of menstrual cycle may lead to functional and emotional morbidities in females leading to difficulty in personal, occupational and social life. Early identification of anxiety and measures to control anxiety can be helpful to reduce this morbidity. This study being a part of larger study and it has taken into consideration only anxiety symptoms where as perceived stress and depression scores are also being considered in larger one.
REFERENCES
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.