 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content Volume 12 Issue 3 - December 2019
Caregiver burden and quality of life among family members of stroke survivors
Devendra Ratnani1, Nishant Sahu2*
1,2Assistant Professor, Department of Psychology, CM medical College, Durg Chhattisgarh, Maharashtra, INDIA. Email: nishin625@gmail.com
Abstract Background: Stroke mortality is higher in Asia than in Western Europe, the Americas, or Australasia, and is more similar to Eastern Europe. Caregivers’ needs are often given low priority in the management of stroke. Objectives: To assess the care giver burden among the family members (primary care giver) of the stroke survivors attending a tertiary care teaching hospital using Zarit caregiver burden scale. To assess the quality of life of care givers among the study population, using the WHO BREF quality of life questionnaire. To assess the correlation between the care giver burden and quality of life among the study population Methodology: The current study was a prospective observational study conducted in the department of psychiatry and the department of general medicine. Care givers of stroke survivors were included. The care giver burden was evaluated by Zarit caregiver burden scale, and the quality of life was estimated by the World Health Organization (WHO) BREF quality of life scale. Data were analysed using IBM SPSS statistical software version 21. Results: Among the care givers,74.17% were females, 64.17% were spouses of stroke survivors and 47.5% were housewives. Environmental health was most affected and social health was least affected. All the components of Zarit caregiver burden scale had a significant negative relationship with psychological, social, environmental and physical domain of quality of life of caregivers. Conclusion: The current study revealed that caregiver burden had a drastic impact on caregiver’s quality of life. More research is required to improve caregiver’s quality of life. Key Word: Caregiver, QOL, Stroke Survivors.
INTRODUCTION A stroke is a clinically defined syndrome of rapidly developing symptoms or signs of focal loss of cerebral function with no apparent cause other than that of vascular origin, but the loss of function can at times be global (applied to patients in a deep coma and those with subarachnoid haemorrhage). Symptoms last more than 24 h or lead to death.1 There are two types of strokes; an ischemic stroke which happens when blood flow to the brain gets interrupted causing damage to the area supplied by that vessel and hemorrhagic stroke which occurs when a blood vessel in the brain ruptures and blood accumulates in the brain and damage to the brain occurs.2 Globally, stroke is a leading cause of mortality and disability, and there are substantial economic costs for post-stroke care.3 In 2016, there were 5·5 million (95% UI 5·3 to 5·7) deaths and 116·4 million (111·4 to 121·4) DALYs due to stroke. The global age-standardised mortality rate decreased by 36·2% (−39·3 to −33·6) from 1990 to 2016, with decreases in all SDI quintiles. Over the same period, the global age-standardised DALY rate declined by 34·2% (−37·2 to −31·5), also with reductions in all SDI quintiles. There were 13·7 million (12·7 to 14·7) new stroke cases in 2016. Global age-standardised incidence declined by 8·1% (−10·7 to −5·5) from 1990 to 2016 and decreased in all SDI quintiles except the middle SDI group. There were 80·1 million (74·1 to 86·3) prevalent cases of stroke globally in 2016; 41·1 million (38·0 to 44·3) in women and 39·0 million (36·1 to 42·1) in men.4 India has been experiencing significant demographic, economic and epidemiological transition during the past two decades. These have resulted in an increase in life expectancy and consequently, an increase in the ageing population.5,6 There is a concerning shift in the overall stroke burden toward younger age groups, particularly in low- and middle-income countries. The epidemic rise in cardiovascular risk factors in young adults in some regions such as Russia, China, and India have contributed to the increase in stroke burden among the younger population. About 12% of strokes in India occur in the community younger than 40 years.7,13 Stroke is an especially severe problem in Asia, which includes more than 60% of the world's population, and many of its countries are “developing” economies. Stroke mortality is higher in Asia than in Western Europe, the Americas, or Australasia, and is more similar to Eastern Europe.14 Advances in stroke rehabilitation have successfully reduced severe disability and institutionalisation, which has increased the number of disabled patients living at home and being supported by caregivers who feel inadequately trained, poorly informed, and dissatisfied with the extent of support available after discharge.15,16 Caregivers play an essential role in supporting people with illness, either acute or chronic. It is crucial to explore caregiver's emotional turmoil as it helps in exploring their burden which can have an impact on the patient's illness and functioning apart from their own.17 The difficulty of care of stroke patients impacts the physical as well as psychological well-being of the caregivers adversely.18 Caregivers’ needs are often given low priority in the management of stroke.19 Current study was conducted to assess the caregiver burden among the family members (primary caregiver) of the stroke survivors attending a tertiary care teaching hospital using Zarit caregiver burden scale with assessment of the quality of life of caregivers among the study population, using the WHO BREF quality of life questionnaire and to assess the correlation between the caregiver burden and quality of life among the study population. RESULTS A total of 110 caregivers of stroke survivors were included in the study. The Following were the baseline characteristics of stroke survivors and their givers. Table 1: Baseline characteristics of the stroke survivors (N=120)
Among the stroke survivors, the mean age was 61.25+ 12.43. There were 6 (5%) people with <40 years age and the proportion of 41-50, 51-60 and 61 and above was 17 (14.17%), 46 (38.3%)and 51 (42.5%) respectively. Among the stroke survivors, 76(63.33%) were Male and remaining 44(36.7%) were female. Among the stroke survivors, 93 (77.5%) were reported Ischemic stroke, and 27 (22.5) reported Hemorrhagic. Majority of the stroke survivors 60(50%) had Hemiparesis, 23 (19.17%) had Hemiplegia and the proportion of people with Paraplegia, Quadriplegia and Hemiparesis/hemiplegia with cranial nerve defects as 11 (9.16%), 6(5%) and 20 (16.67%) respectively. (Table 1) Table 2: Baseline characteristics of the care givers (N=120)
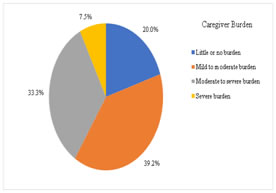
Among the care givers, the mean age was 48.25+ 7.89 years. There were 17(14.17%) people with <40 years age and the proportion of 41-50, 51-60 and 61 and above was 64(53.33%), 26 (21.67%) and 13 (10.83%) respectively. Among the care givers, 31(25.83%) were Male and remaining 89(74.1%) were female. Among the care givers, 77 (64.17%) were spouse of stroke survivors, 26 (21.67%) were children of stroke survivors, and the proportion of siblings and other family members of stroke survivorswas 8 (6.67%) and 9 (7.5%). Among the care givers, 57(47.5%) were housewife, 48(40%) were employed and 15(12.5%) were retired / unemployed. (Table 2) Figure 1: Pie chart of caregiver burden in the study population (N=120) Among the study population, according to Zarit Burden inventory schedule score 24(20%) were with Little or no burden and 47(39.17%) were with Mild to the moderate burden, 40(33.33%) were with Moderate to severe burden and only 9(7.5%) were with Severe burden. (Figure 1) For the purpose of assessing the association between the care giver burden and quality of life, we have combined all the three categories with care giver burden and compared it with the caregivers without any burden. Table 4: Impact of caregiver burden on quality of life among caregivers
Among the caregivers with burden mean Physical score was 19.48 ± 2.38, and it was 24.37 ± 1.97 without burden. Among the caregivers with burden mean Psychological score was 18.97 ± 1.92, and it was 21.32 ± 2.07 without burden. Among the caregivers with burden mean Social score was 6.23 ± 2.31, and it was 9.23 ± 1.86 without burden. Among the caregivers with burden mean Environment was 26.13± 4.16, and it was 30.18 ± 4.12 without burden. (Table 4)
DISCUSSION Stroke continues to be a leading cause of death and long-term disability in adults worldwide. In India and other developing countries, an alarming increase in the incidence of stroke has been observed. Stroke is a crisis for the family because of the sudden onset of nature and multiple impairments in survivors.22 While much attention had been paid to the incidence and prevalence of stroke, there have been much fewer studies focusing on the long-term consequences and the need for ongoing assistance and caregiving. Literature search has revealed some reports from the developed countries, but hardly any from the developing countries.23 The current study showed that for stroke survivor’s female caregivers were in majority. A study conducted to understand the caregivers (CGs) stress in stroke survivors had Majority of the 74.62% female caregivers.24 The most shared relationship between caregivers and stroke survivors was spousal relationship. In studies conducted by Das, S et al25, and Morimoto, T et al26, 59 (30%) and 52(52%) of caregivers were wife of the stroke survivors which depicted spousal relationship was predominant than other relationships. Stroke survivors in our study majorly had ischemic stroke and hemiparesis as disability. A study was done to investigate informal caregivers’ burden, and strains of caring for stroke patients had 96 had ischaemic stroke similar to our study results.27 Our results stated that homemakers were mainly involved as caregivers for stroke survivors. As per Zarit Burden inventory schedule score majority represented mild to moderate burden. Total of 65% of CGs graded their burden as moderate to severe in study conducted by Menon B et.al.24 Caro CC et al28, in their results had ZBIS 29.6 and moderate burden. The quality of life is a multiple dimension which mainly consists of physical, psychological, social and environmental health of an individual. In present study, the quality of life of caregivers were classified in each domain wise. Among all the four domain, environmental health was most affected and social health was least affected. All the components of Zarit caregiver burden scale had a significant negative relationship with psychological, social, environmental and physical domain of quality of life of caregivers. Rawat M et al29, found that the most of the caregivers were in severe level of burden in most of the caregivers and similar to our study findings a significant negative correlation between quality of life and burden scores of caregivers.
CONCLUSION The current study revealed that caregiver burden had a drastic impact on caregiver’s quality of life. Priority towards caregiver’s well-being is neglected. More attention should be given to spouses of stroke survivors as they are closely related and dependent on each other. Basic Training for caregivers should be provided to reduce stress and efficiently carry out activities related to stroke survivors. More interventions and research work are required to improve quality of life of caregivers and reduce the caregiver burden.
REFERENCES
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.