 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 4 Issue 2 - November 2017
Duration, onset, severity of alcohol dependence in patients and its relation to quality of life of their caregivers
Murali Krishna V1, Gautham Tialam2*, Raghuram Macharapu3
1Resident, 2Assistant Professor, Department of Psychiatry, Kakatiya Medical College, Warangal, Telangana, INDIA. 3Associate Professor, Department of Psychiatry, Mamata Medical College, Khammam, Telangana, INDIA. Email: gautham.tialam@gmail.com, dr.muralikrishna111@gmail.com
Abstract Objective: To find out the Quality of Life in various domains in caregivers of patients with Alcohol dependence syndrome and its relation to onset, duration, severity of alcohol dependence. Materials and Methods: The study was cross sectional, conducted in Mamata Medical College, Khammam, from September 2016 to March 2017. Our study sample contains 50 alcohol dependent patients who admitted in psychiatry ward at, Mamata General Hospital, and their care giversare included in the present study. Results: Quality of life is more affected in physical and Psychological domain and followed by social and environmental domain. Analysis of different domains of quality of life in different age groups of patients shows low score in social and environmental domains in 46-60 years age group. These values were not found to be statistically significant (p<0.05). In care givers low scores are obtained in physical and environmental domains in 46-60 years age group. These values were not found to be statistically significant (p<0.05). The physical, psychological and environmental domains of caregivers of severe alcohol dependent individuals are significantly lower than caregivers of mild and moderate alcohol dependent individuals. Conclusion: Care givers of severe alcohol dependent patients have significantly lower quality of life. As the duration of alcohol dependence increases, quality of life is decreased. Key Words: Quality of life, caregivers, alcohol dependent, duration of alcohol dependence.
An uncontrollable, overwhelming and irresistible desire to consume alcohol was described by Benjamin Rush in 1784.1 Alcohol craving and withdrawal symptoms were integral parts of the concept of addiction and of the destructive effects of alcohol consumption promoted by the temperance movement in the 19th century.2 There was, however, a fundamental difference to current concepts of alcoholism: the temperance movement suggested that anyone who consumed excessive amounts of alcohol would suffer from alcohol-related problems and did not suggest that alcoholism could affect certain specifically vulnerable individuals primarily.2,3 Dependence syndrome (Alcohol Dependence syndrome) is a cluster of physiological, behavioral, and cognitive phenomena in which the use of a substance (alcohol) takes on a much higher priority for a given individual than other behaviors that once had greater value.4 Alcohol dependence, a common psychiatric disorder in the general population, has a significant impact on health. In recent years, alcohol dependence has become a major social and personal menace in most societies. In northern India including Delhi, the 1-year prevalence of alcohol use has been estimated as 25 to 40% in the general population, whereas in southern India, this rate has been estimated as 30 to 50%. In southern India, the prevalence of alcohol use is higher among people of lower socio-economic status and those with lower levels of education.4 A large-scale survey over 32,000 people performed in 2001 in India found alcohol use rates of 20 to 38% in males and 10% among females.5 Some people are more likely to experience the consequences of alcohol use. These tend to be male6,7, having high perceived stress and anxiety with dissatisfaction and poor quality of life, lack of social support, economic strains, and chronic stress.8 Das, Balakrishnan, and Vasudevan reported that in a developing country like India, over 20% of all disability-adjusted life years are lost chiefly because of poor health status of the people, marked nutritional deficiencies, and widely prevalent alcohol addiction.9 Alcohol addiction will complicate a situation involving a caregiver and someone in his or her care. Being a caregiver is already a difficult, draining, stress-producing and often heartbreaking job. Alcohol addiction on the part of the patient or the caregiver will make the job much harder and make the situation more stressful and unpleasant for all involved. The impact of alcohol problems on family members of the alcohol dependence individuals is wide-spread; virtually it can penetrate into every area of life, e.g., physical and psychological health, finances, employment, social life and relationships. Alcoholism is a major public health problem around the world (WHO, 2010).The magnitude of the problem in our country is considerable given that India has the second largest population in the world, with 33% of its population consuming alcohol according to study conducted by Gururaj, and coworkers.10 Caregiver burden can be conceptualized as both the tasks that need to be done in the course of care giving and the way in which the caregiver appraises the performance of these tasks.11 Care giving tasks take many different forms. For example, caregivers may assist care recipients with activities of daily living, prepare meals, perform housekeeping tasks, run errands, or manage finances. Caregivers may also be responsible for providing care after a debilitating illness or for monitoring for a person suffering from dementia. A number of external factors, including caregiver personality, social support network, status in the family, and other responsibilities impact how an individual appraises their care giving responsibilities.(12,13) For example, a large body of literature has found that caregivers with a strong social support network report less burden than those who lack social support.14,15,16 regardless of the number or type of care giving tasks. A positive interpretation of the care giving role has been shown to be similarly protective.17 Therapeutic approaches to decrease psychosocial co-morbidity in wives of alcohol dependence syndrome has also been studied.18,19,20 the success of these attempts can be evaluated by means of “Quality of Life” (QOL). WHO defines “Quality of life” as individuals’ perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards and concerns. Measurement of health and the effects of health care most include not only an indication of changes in the frequency and severity of diseases but also an estimation of well being and this can be assessed by measuring the improvement in the quality of life related to health care.21 So, in summary we need more research into the area of psychiatric morbidity and QOL in wives of alcohol dependent patients. A precise understanding of the problems, pattern, risk factors, maintaining factors etc. is essential for any interventions in this area. This study is an attempt in this direction.
MATERIALS AND METHODS Place of Study: Study was conducted inMamata general hospital, Khammam, Telangana. Study Period: The study undertaken during July 2016 to February 2017 in the department of psychiatry following the college’s ethical committee approval. Study Sample: The study sample consists of 5050 alcohol dependent patients who admitted in psychiatry ward at, Mamata General Hospital, and their care givers are included in the present study, who are willing to participate in the study. Study Design: Cross sectional. Inclusion Criteria: Availability of caregivers, Age of patient and caregiver should be between 15-60years, Both should be physically fit to answer the questions Exclusion Criteria: Patients without caretaker who can give reliable and adequate information, Those who did not give consent for the study. Materials: Socio-demographic and clinical profile sheet (Annexure-I) The socio-demographic and clinical profile sheet was administered by the investigtator to record certain variables such as age, sex, marital status, duration of marriage, type of family, locality, income and Clinical variables viz, age at onset of substance use, age at dependence and duration of dependence. World Health Organization Quality of Life (WHOQOL) questionnaire22 (Annexure- II) The WHOQOL-BREF (field trial version) was constructed by WHO in 1995. It consists of four domains. The 4 domains are physical, psychological, social relationship and environmental domains. Each domain consists of 7,6.3 and 8 questions respectively. there are also 2 single items that are examined separately. Q1 is about an individual’s overall perception of quality of life and Q2 is about his or her perception of overall health, it is easy to administer and has been validated. Domain scores are scaled in positive direction i.e., higher scores donate higher quality of life. Severity of alcohol dependence questionnaire (SOADQ)23 (Annexure-V) It is a short easy to complete, self-administered, pencil and paper, 20-item questionnaire designed to measure the severity of dependence on alcohol. There are 5 subscales with 4 items in each. These are physical withdrawal, affective withdrawal, withdrawal relieve drinking, alcohol consumption and rapidity of reinstatement. It has a test re-test reliability of 0.95 and proven content, criterion and construct validity. The maximum score is 60. Statistical Analysis: The data obtained was analyzed using Statistical Package for the Social Sciences (SPSS), Version 16. student-t test and ANOVA test used.
RESULTS Table 1: Quality of life in caregivers of patients with alcohol dependence syndrome
Quality of life is more affected in physical and Psychological domain and followed by social and environmental domain.
Table 2A: Age distribution of patients with Quality of life in caregivers
Analysis of different domains of quality of life in different age groups of patients shows low score in social and environmental domains in 46-60 years age group. These values were not found to be statistically significant (p<0.05). Table 2B: Age distribution with Quality of life (in caregivers)
In care givers low scores are obtained in physical and environmental domains in 46-60 years age group. These values were not found to be statistically significant (p<0.05).
Table 3: Relationship between Severity of alcohol dependence in patients with Quality of life in their caregivers
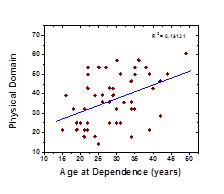
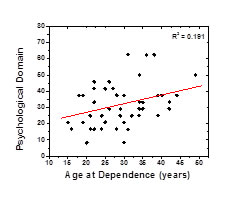
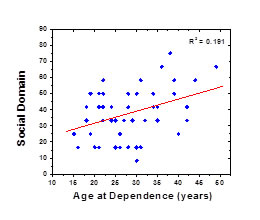
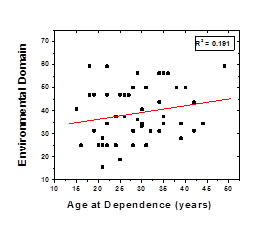
The physical, psychological and environmental domains of caregivers of severe alcohol dependent individuals are significantly lower than caregivers of mild and moderate alcohol dependent individuals. Age at dependence Vs Domains of Quality of life of wives
Figure 1A: Figure 1B: Age at dependence Vs Physical Domain Age at dependence Vs Psychological Domain Figure
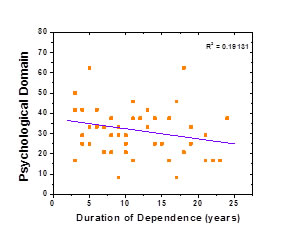
Figure 2A: Figure 2B: Duration of dependence Vs Physical Domain Duration of dependence Vs Psychological Domain
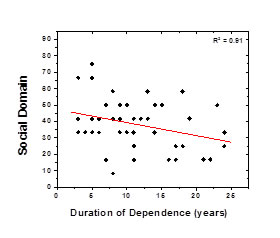
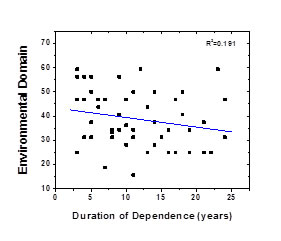
Figure 2C: Figure 2D: Duration of dependence Vs social Domain Duration of dependence Vs Environmental Domain DISCUSSION In the present study, average age of patients and caregivers is around 40, where generally people settle in their career and form strong psychosocial bonding with society. Because of this alcohol dependent pattern, patients and their care givers life will be disturbed in psychosocially and financially which in turn affects the society as alcohol persons when they are intoxicated they are prone to involve in illegal activities which can disturb the balance of society. Quality of life is an important parameter that provides an insight into how a disorder impacts life of those affected. In present study quality of life in caregivers of patients with alcohol dependence syndrome is calculated. The score on QOL-1 (Overall Quality of life) is calculated by taking the patient’s information on his/her quality of life. The score on QOL-2 (General Health) is measured by asking the patient that how he/she is satisfied with his/her health. The physical domain has seven items i.e., pain, energy, sleep, mobility, activity, medication and work. The psychological domain has six components i.e., positive feeling, think esteem, body, negative feeling and spirituality. Social domain has only three items i.e., relaxation, support and sex. Environmental domain has eight components i.e., safety finances, services, information, leisure, environment and transfer. Analysis of different domains of quality of life in different age groups of patients shows low scores in social and environmental domains in 46-60 years age group, however these values were not found to be statistically significant. In caregivers low scores are also obtained in physical and environmental domains in 46-60 years age group. These scores are not found to be statistically significant in all domains of quality of life. The findings of our study are broadly in agreement with that of Kreider and his coworkers.24 Such low scores in all domains in higher age groups can be considered as influences of the chronicity of the illness as well as increasing social rejection with passage of time. In our study analysis concerning the severity of alcohol dependents and different domains of quality of life of caregivers was done. The severity of alcohol dependence was divided in to three subgroups depending upon the scores obtained on Severity of Alcohol Dependence questionnaire (SADQ) used. Scores lower than 16 indicate mild dependence, scores between 16and 30indicate moderate dependence and 31 or higher indicate severe alcohol dependence. The scores obtained on domains of quality of life of caregivers of severe alcohol dependent individuals was found to be low physical, psychological, social and environmental respectively compared to domains of quality of life of caregivers of mild and moderate group of alcohol dependent individuals. The physical, psychological and environmental domains of caregivers of severe alcohol dependent individuals are significantly lower than caregivers of mild and moderate alcohol dependent individuals. Such positive association between severity of alcohol dependence in patients and low scores obtained in different domains of quality of life of caregivers is an obvious phenomenon. Most of the severe alcohol dependence patients start taking alcohol after getting up from bed and continues to drink more in amounts throughout day. It leads to definite declining health and occupational status. Figure no.1 exhibits age of dependence of our study sample on x axis and individual domain of quality of life on y axis. Mean age at dependence was found to be 28.66 (±7.97601) years. With increased age at dependence of husband, quality of life deteriorates in caregivers. Epstein and coworkers25 conducted a longitudinal study on marital functioning of alcoholics according to different alcohol typologies. The samples of study were alcoholic males and their female partners. Four typologies-including Type One/Two, In-Home/Out-of-home, steady/Episodic, and Early/Late Onset-were tested for replicability and discriminant validity before linking them to marital functioning. Discriminant validity was found only for the Early (59%) versus Late (41%) onset typology. At baseline, Early-onset couples reported more marital instability and the females in these couples were more distressed. During treatment, Early-Onset couples reported higher daily marital satisfaction than Late-Onset couples. Regardless of age of onset, males reported higher marital satisfaction than their spouses during treatment but their satisfaction did not increase during treatment. Female partners marital satisfaction increased during treatment. Female partners of Late-onset males reported particularly low marital satisfaction during treatment. Different predictors of marital satisfaction for males and females were found within each subtype. For female partners of Early-Onset alcoholics, psychological distress unrelated to her partner’s drinking severity was most associated with her own marital satisfaction, whereas marital adjustment of female partners of Late-Ons et al coholics was most associated with the males level of perceptual accuracy regarding her needs. This pattern was reversed for the males; marital adjustment of Early-Onset alcoholics was most associated with his partner’s perceptual accuracy of his needs, whereas marital functioning of Late-Onset alcoholics was best accounted for by his own psychological distress. Figure no 2 exhibits duration of dependence of our study sample. Average age at duration of dependence was found to be 11.46(±6.18164) years This is more negatively correlated in physical (r=-0.42193) and social (r=-0.32163) domains quality of life. Tempier and co-workers (26) conducted a retrospective study of female spouses of male at risk drinkers. The objective was to determine the mental health of female spouses living with a male lifetime at-risk drinker, also to examine the relationship between male lifetime at-risk drinkers (aged 30-54years) and the psychological distress of their nondrinking female spouses.
CONCLUSION
LIMITATIONS Study sample was collected from only one tertiary care hospital, which was the major limitation of the study and further research can be conducted, so results cannot be generalised to the population.
REFERENCES
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 1C: Figure 1D:
1C: Figure 1D: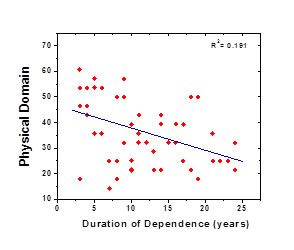
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.