 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 6 Issue 2 - May 2018
Comparison of female sexual functions among various psychiatric morbidities
Sajal Ashish Nag1*, Jyoti Shetty2
1Jr. Resident, 2Professor and HOD, Department of Psychiatry, Bharati Vidyapeeth Medical College and Hospital, Dhankawadi, Pune, Maharashtra, INDIA. Email: sajal1912@gmail.com
Abstract Background: The prevalence of sexual dysfunctions is higher in females with mental disorders, particularly those treated with psychotropic medications. Psychiatric disease is the most important risk factor for women’s sexual dysfunction. Aim: To assess sexual dysfunction in female patients with major psychiatric morbidities such as schizophrenia, bipolar affective disorder and depression. Material and Methods: A total of 13 female patients with psychiatric morbidities were assessed for sexual dysfunction, and screened and diagnosed using the ICD 10 criteria, CSFQ-F-C, CGI-S scales and FSFI. Results: There were4 (31%) cases of schizophrenia, 5 (39%) cases of Unipolar depression, 2 (15%) cases of bipolar depression and 2 (15%) cases of Mania. Mean score in schizophrenia and depression was low(p<0.05) in all the function domains. Mean scores were lowest in cases with depression. However, in mania cases, the mean scores were higher in domains of orgasm and satisfaction. Conclusion: Knowledge of sexual dysfunctions in females with psychiatric morbidities, help the clinicians to make needed inquiries and treatment recommendations. Key Words: Psychiatric morbidities, sexual dysfunction, females, schizophrenia, depression.
INTRODUCTION Sexual dysfunction refers to difficulty experienced by an individual or a couple during any stage of normal sexual activity, including desire, arousal or orgasm. The prevalence of sexual dysfunctions is higher in females with mental disorders, particularly those treated with psychotropic medications. Psychiatric disease is the most important risk factor for women’s sexual dysfunction.1,2 Both men and women experience these phases, although the timing usually is different. Female sexual dysfunction takes different forms, including lack of sexual desire, impaired arousal, inability to achieve orgasm, or pain with sexual activity.3The relationship between sexual dysfunction and psychotic disease in women is poorly understood. As with women experiencing depression and anxiety, women with schizophrenia and schizophrenia spectrum disorders have a very high burden of sexual dysfunction, with 60%–80% of women being affected.4-6 The present study thus aimed to assess sexual dysfunction in female patients with major psychiatric disorders such as schizophrenia, bipolar affective disorder and depression.
MATERIAL AND METHODS In this hospital based cross sectional study a total of 13 female patients with major psychiatric disorders, diagnosed as per International Classification of Diseases (ICD-10) and started on treatment 6 months prior to study inclusion were studied for sexual dysfunction. Inclusion Criteria
Exclusion Criteria
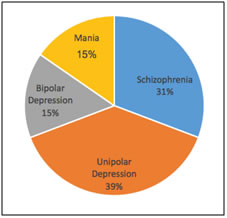
Methodology: Patients were informed about the study and a written informed consent was taken. All female patients were interviewed face to face using the diagnostic tools. Approval from our institutional review board was taken before start of the study. The patientsr eceiving treatment for major psychiatric disorder i.e. schizophrenia/bipolar affective disorder/depression in the outpatient department as well as those admitted in the indoor ward were assessed for sexual dysfunction, and screened and diagnosed using the ICD 10 criteria,7 CSFQ-F-C,8CGI-S scales9and FSFI.10 Diagnosis of all the patients was confirmed by consulting Psychiatrist at Psychiatry Department, Tertiary care Hospital. Statistical Analysis: All the data was analyzed statistically by SPSS software ver. 21 using appropriate test. Qualitative data was presented as frequency and percentages and analyzed using Chi-square test while quantitative data was presented as means and SD. In the present study 13female cases of major psychiatric illness were studied for sexual dysfunction. Majority of the patients were in their 3rd and 4th decade. As per ICD-10 classification, we had 4 (31%) cases of schizophrenia, 5 (39%) cases of Unipolar depression, 2 (15%) cases of bipolar depression and 2 (15%) cases of Mania.
Figure 1: Distribution of female patients with psychiatric morbidities
Sexual dysfunction among females was computed by using Female Sexual Function Index. Mean score in schizophrenia and depression (p<0.05) in all the function domains like desire, arousal, lubrication, orgasm, satisfaction and pain. Mean scores were lowest in cases with depression. Sexual dysfunction among females was computed by using Female Sexual Function Index. Mean score in schizophrenia and depression (p<0.05) in all the function domains like desire, arousal, lubrication, orgasm, satisfaction and pain. Mean scores were lowest in cases with depression.
Table 1: Comparison of Female sexual functions as per FSFI score among various psychiatric morbidities
Female sexual functions were also evaluated using Changes in Sexual Functioning Questionnaire for females (CSFQ-M). Sexual desire and orgasmic satisfaction was lower in depression cases than schizophrenia. Over two third of the cases with depression showed scores below cut-off levels in most domains, while none of the cases with mania showed scores below cut-off levels in any of the domains. Table 2: Comparison of Female sexual functions as per CSFQ score among various psychiatric morbidities
DISCUSSION Women with psychotic illness experience a variety of dysfunctions, including impaired arousal, delayed or absent orgasm, low frequency of sexual activity and decreased sexual satisfaction.11-13 Recent research suggests that both partnered and individual desire may be similar in women with psychotic illness and age-matched healthy women.14 The pathophysiology of sexual dysfunction in psychotic illness remains poorly understood, particularly with regards to psychosocial factors. Potential etiologies of sexual dysfunction include antipsychotic medications, positive and negative symptoms of psychosis, interpersonal difficulties, stigmatization, sexual trauma and somatic concerns. Researchers identifiedthe strong link between depression and women’s reduced interest or desire for partnered sex and epidemiological studies confirm depression’s negative effects upon orgasmic experience.15 Sexual dysfunction among females was computed by using Female Sexual Function Index (FSFI). Mean score in depression were lower than the original study controls (p<0.05) in all the function domains like desire, arousal, lubrication, orgasm, satisfaction and pain. As per, Changes in Sexual Functioning Questionnaire (CSFQ), Sexual desire was significantly affected in both males and females while in females sexual pleasure and orgasm domains were also affected. The prevalence of sexual dysfunctions is higher in persons with depression, particularly those treated with psychotropic medications. Zemishlany Z et al reported sexual dysfunction in up to 78% of individuals with depression treated with antidepressants.3 Casper et al, found sexual dysfunction in 72% of cases with unipolar depressed and most of these cases experienced loss of sexual interest. Increasing severity of depression was also observed to be associated with loss of libido.16 As per FSFI, mean score in schizophrenia were lower than the controls (p<0.05) in all the function domains. As per CSFQ, sexual pleasure and excitement was affected in females with schizophrenia. Patients suffering from schizophrenia are prone to experience sexual dysfunction with few interpersonal relationships and lack of sexual experience. Negative symptoms of the disorder severely harm the ability to enjoy sexual life. In addition, these patients face difficulties in establishing relationships due to recurrent psychotic episodes, obesity and low self-esteem. Few studies have investigated the prevalence of sexual dysfunction amongst schizophrenia patients. Zemishlany Z et al in their study reported sexual dysfunction in as many as 60% of patients with schizophrenia.3 In a recent study by Macdonald et al observed atleast one sexual dysfunction was reported by 96% of women with schizophrenia. Female patients reported less enjoyment than the control group (46 vs. 5%).17 As per IIEF and FSFI, mean scores in females with mania cases was higher than controls showing increased orgasm and satisfaction among females.
CONCLUSION Sexual dysfunctions among women with psychiatric morbidities are likely to be multifactorial, with contribution from medications, the symptoms of psychosis, somatic illness and the sociocultural effects of severe mental illness. More research needs to be conducted to understand the complex pathophysiology of the sexual dysfunction seen among women with psychosis. Knowledge of sexual dysfunctions, help the clinicians to make needed inquiries and treatment recommendations.
REFERENCES
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.