 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 10 Issue 2 -May 2019
Comparison of recovery and emergence characteristics of patients in two groups of desflurane and sevoflurane after paediatric general anaesthesia
Ambika Bandagi1*, G K Nikam2, Shailesh Chauhan3
1Junior Resident III, 2Associate Professor, 3Professor and HOD, Department of Anaesthesiology, SRTR GMC Ambajogai, Beed, Maharashtra. Email: ambika.avb@gmail.com
Abstract Background: A child’s emergence behaviour from general anaesthesia is important to both the Anaesthesiologist and the parent. Often times, patients are agitated upon emergence and during the initial recovery period. Emergence agitation occurs most frequently during the initial 10 minutes of recovery and has been defined as non-purposeful restlessness, agitation, thrashing, crying or moaning, disorientation and incoherence. Aim and objectives: To compare the recovery and emergence characteristics of patients in two groups of Desflurane and sevoflurane after paediatric General Anaesthesia. Materials and method: In the present study total 100 Paediatric patients of either gender of age group of 5-12 years with ASA I or II and posted for minor surgical procedures of head, neck, face and abdomen surgeries under general anaesthesia were enrolled. Patients were randomly divided into 2 groups of 50 patients each according to a computer-generated random numbers table. Desflurane Group: Anaesthesia induced using inj. Propofol (2mg/kg) and maintained with 60% N2O and 40% O2 and desflurane. Sevoflurane Group: Anaesthesia induced using inj. Propofol (2mg/kg) and maintained with 60% N2O and 40%O2 and sevoflurane. Time required for Regular Breathing, Response to pain, Obey commands, Limb lift, Extubation, Shift to PACU and discharge from PACU that is time to Achieve PARS ≥ 9 (post anaesthesia recovery score of Aldrete and Kroulik) were recorded for both the groups and compare. Results: Age, sex, weight and the duration of surgery were comparable in both the groups. The mean time taken for the patients to breathe regularly following discontinuation of anaesthesia was 4.8 minutes and 6.74 minutes in desflurane and sevoflurane group, respectively. The mean time taken for the patient to respond to painful stimulus following discontinuation of anaesthesia was 5.42 minutes and 9.37 minutes in desflurane and sevoflurane group, respectively The mean time taken by the patients to obey to vocal commands was found to be 6.07 minutes and 10.35 minutes in desflurane and sevoflurane group, respectively. The mean time taken by the patients for spontaneous eye opening in desflurane and sevoflurane group was found to be 6.93 minutes and 11.27 minutes, respectively. Mean time taken by the patients for lifting their limbs was found to be 7.68 minutes and 11.96 minutes in desflurane and sevoflurane group, respectively. Conclusion: we conclude that Desflurane had rapid emergence, recovery from anaesthesia and early discharge from PACU when compared with sevoflurane. Key words: recovery and emergence characteristics, paediatric General Anaesthesia, Desflurane and sevoflurane
INTRODUCTION Inhalational anesthetics are the most common drugs used for the provision of general anaesthesia. Addition of only a fraction of a volatile anesthetic to the inspired oxygen results in a state of unconsciousness and amnesia. When combined with intravenous adjuvants, opioids and benzodiazepines, a balanced anesthetic technique is achieved that results in analgesia, further sedation or hypnosis, and amnesia. Paediatric patients, who because of their need for extensive treatment, acute situational anxiety, pre-cooperative or uncooperative age-appropriate behavior, immature cognitive functioning, disabilities, or medical conditions, it is more cost-effective, efficient, and humane to treat these children with general anaesthesia.1 The popularity of the inhaled anesthetics for surgical procedures is because of their ease of administration and the ability to reliably monitor their effects with both clinical signs and end-tidal concentrations. There are two aspects of general anaesthesia that involve inhalants: the induction phase and the maintenance phase. The Induction Phase is defined as the time period when the patient initially receives anesthetic medication until they become unconscious. The Maintenance Phase is defined as the period of time from intubation until the surgery is complete and the anesthetic gases have been turned off. The emergence time from general anaesthesia is defined as the end of the administration of anesthetic until extubation.2 One of the major factors that determine speed of recovery from anaesthesia is the choice of anaesthetic technique. An ideal general anaesthetic, for the ambulatory patients, should provide smooth and rapid induction, optimal operating conditions, and rapid recovery with minimal side effects like nausea, vomiting, bleeding and postoperative pain. Inhaled anaesthetics allow rapid emergence from anaesthesia because of easy titrability with inherent neuromuscular blocking effects that make them more suitable for ambulatory anaesthesia.3 The availability of less soluble inhalational anaesthetics such as sevoflurane and desflurane made us rethink about the selection of volatile anaesthetics for outpatient surgical procedures. Given the low blood: gas partition coefficient of sevoflurane and desflurane, faster emergence from anaesthesia is expected to compared to traditional inhalational anaesthetics.4 Generally, sevoflurane is the inhalant used for induction because it is not a respiratory irritant and it has a less pungent odor. 5,6,7,8 It has been shown to be safe and highly efficacious. It has a rapid uptake and elimination because of its low blood-gas partition coefficient. Sevoflurane can be used as a maintenance gas as well.5,6,8,9 A child’s emergence behaviour from general anaesthesia is important to both the Anaesthesiologist and the parent. Often times, patients are agitated upon emergence and during the initial recovery period. Emergence agitation occurs most frequently during the initial 10 minutes of recovery and has been defined as non-purposeful restlessness, agitation, thrashing, crying or moaning, disorientation and incoherence. 9,10,11 Both sevoflurane and desflurane have shorter emergence times compared to isoflurane based anaesthesia techniques. Because of its pharmacological properties, desflurane appears to yield a rapid early and intermediate recovery compared with sevoflurane. However, the results of different studies have been conflicting. Also, desflurane has only recently become available in India and has yet not been studied for daycare surgery in Indian pediatric population.4 MATERIALS AND METHOD The present randomised, prospective; single-blind study conducted over a period of 2 years from November 2016 – October 2018 in tertiary care hospital. Approval for the study was obtained from the Institutional Ethics Committee. Permission for assessing the patients and handling their case record papers was also obtained from respective department heads. Sample size was calculated based on Master 2.0 software with alpha error of 5% and power of 80%. Sample size was found to be 50 per group; total 100 Paediatric Patients satisfying the inclusion criteria posted in the operation theatre for various surgical procedures under general anaesthesia during the study period. Inclusion Criteria:
Exclusion Criteria:
The patient’s parents or legal guardians consenting to participate were explained in detail. A detailed history was obtained and thorough physical examination was carried out. Complete blood count, renal function test, blood grouping/typing, random blood sugar, electrocardiograph and chest x-ray were done. Patients were randomly divided into 2 groups of 50 patients each according to a computer-generated random numbers table.
The Heart rate, systolic blood pressure, diastolic blood pressure, Mean arterial pressure and SPO2 with end tidal carbon dioxide was continuously monitored at pre induction, post induction, after intubation, 5 minutes after that and every 10 minutes till the end the of surgery and at 15th minute postoperatively. Time required for Regular Breathing, Response to pain, Obey commands, Limb lift, Extubation, Shift to PACU and discharge from PACU that is time to Achieve PARS ≥ 9 (post anaesthesia recovery score of Aldrete and Kroulik) were recorded for both the groups and compare. Statistical analysis was done using Microsoft Excel 2010. Analysis was done and expressed in terms of mean and standard deviation and standard error of mean. Analysis of variance (ANOVA) test, t-test were used to analyze the data. p<0.05 was considered as statistically significant. Results were represented in tables and graphs. RESULTS Table 1: Distribution of patients according demographic details
The mean age of patients was 8.44 years in Desflurane group and 7.98 years in Sevoflurane group. The mean weight of patients in desflurane group was 19.3 kg and in sevoflurane group it was 18.46 kg and the difference was not statistically significant; hence both the groups were comparable in terms of weight of patients. It was seen that there were 18 males in desflurane group and 26 in sevoflurane group and there was no statistically significant difference between the groups (p>0.05). The mean total duration of surgery in desflurane group was 62.3 minutes and in the sevoflurane group it was 68.7 minutes and the difference was not statistically significant. The mean total duration of anaesthesia in Desflurane group was 67.44 minutes and in the Sevoflurane group it was 73.9 minutes and the difference was not significant and thus both the groups were comparable in both the groups. Table 2: Baseline profile of parameters in two treatment groups
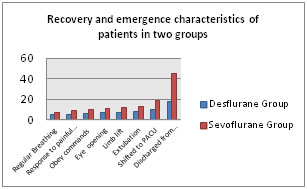
The baseline mean heart rate, systolic blood pressure, diastolic blood pressure, mean arterial pressure, SPO2 and ETCO2 values in two treatment groups was compared. All the parameters in the groups were in normal range and were respectively comparable since there was no statistically significant difference between the two groups (p>0.05). Table 3: Recovery and emergence characteristics of patients in two groups
The mean time taken for the patients to breathe regularly following discontinuation of anaesthesia was 4.8 minutes and 6.74 minutes in desflurane and sevoflurane group, respectively. On statistically analyzing the data, p value was 0.001, hence statistically significant. The mean time taken for the patient to respond to painful stimulus following discontinuation of anaesthesia was 5.42 minutes and 9.37 minutes in desflurane and sevoflurane group, respectively and the difference was statistically significant. The mean time taken by the patients to obey to vocal commands was found to be 6.07 minutes and 10.35 minutes in desflurane and sevoflurane group, respectively. The difference was statistically significant with sevoflurane group taking longer time to obey commands as compared to desflurane group. The mean time taken by the patients for spontaneous eye opening in desflurane and sevoflurane group was found to be 6.93 minutes and 11.27 minutes, respectively. The difference was statistically significant with sevoflurane group taking longer time to obey commands as compared to desflurane group. It was observed that mean time taken by the patients for lifting their limbs was found to be 7.68 minutes and 11.96 minutes in desflurane and sevoflurane group, respectively and the difference was statistically significant. The time taken for extubation in sevoflurane group was significantly longer (p <0.005) when compared to the desflurane group. The time taken for patients to be shifted to PACU in sevoflurane group (8.87 minutes) was significantly longer when compared to the desflurane group (9.82 minutes). The time taken for patients to be discharged from PACU in sevoflurane group was significantly longer (p <0.005) when compared to the desflurane group. Mean time taken for the discharge was 17.4 minutes and 45.1 minutes in desflurane and sevoflurane group respectively.
DISCUSSION The present study was planned to compare the recovery and emergence characteristics of patients in two groups of Desflurane and sevoflurane after paediatric General Anaesthesia. On analyzing the demographic profile, the distribution of age and weight of the patients in both the groups were comparable. Also, there was no significant difference in the ASA PS status and duration of anaesthesia and surgical duration between the two groups. The time taken to achieve desired end tidal concentration was comparable in both the groups. This was similar to S. Gergin et al study.12 The time to spontaneous breathing, response to pain, tame to obey commands and eyeopening , time to limb lift and hand grip, time to extubation, time to discharge from PACU were shorter in the desflurane group compared to sevoflurane group. Post anaesthesia recovery score of Aldrete and Kroulik greater than or equal to 9 was achieved earlier in the desflurane group. In the desflurane group, time taken for regular breathing in a mean time of 4.8±0.93minutes after the discontinuation of the anaesthetics whereas it took a mean of 6.74±1.22 minutes in the sevoflurane group. The time taken for response to painful stimulus was achieved in a mean time of 5.42±1.06 minutes in the desflurane group whereas in the sevoflurane group it took a mean of 9.37±1.67 minutes. This was similar to the S Gergin et al12 study which showed a faster emergence in Desflurane group. In desflurane group, time taken to obey commands in mean time of 6.07±1.16 minutes whereas it took a mean time of 10.35±1.68 minutes in sevoflurane group. McKay RE et al13 concluded in their study that the time taken to response to verbal commands was significantly longer with sevoflurane when compared to Desflurane. The time taken for eye opening was achieved in a mean time of 6.93±1.22 minutes in the desflurane group whereas in the sevoflurane group it took a mean of 11.27±1.57 minutes. In desflurane group, time taken to limb lift in mean time of 7.68±1.25 minutes whereas it took a mean time of 11.96±1.57 minutes in sevoflurane group. The patients in the desflurane group were extubated earlier than those in the sevoflurane group. The patients in the desflurane group were extubated in a mean time of 8.27±1.27 minutes whereas those in the sevoflurane group took 13.13±1.89 minutes. Meta analysis, conducted by Macario A et al14, of 22 studies done on a total of 746 patients who revieved sevoflurane and 752 who received desflurane were compared about their postoperative recovery characteristics. It was found out that the patients receiving desflurane followed commands, were extubated, and were oriented 1.0-1.2 minutes earlier than those receiving sevoflurane. The time taken for patients to be shifted to PACU was achieved earlier in the desflurane group (9.82±0.79 minutes), whereas for Sevoflurane, it took 18.87±1.97 minutes. The time taken for discharge from PACU that is The mean duration for PARS >10 was achieved in a mean of 17.44±1.66 minutes in desflurane group which was earlier than sevoflurane (45.08±6.22 minutes). This was similar to the S Gergin et al12 study which showed a faster recovery in Desflurane group. This was similar to Isik Y et al15 study which concluded PARS >10 was significantly rapid in and its 11 minutes and 12.5 minutes in Desflurane group and Sevoflurane group. L.E. C. De Baerdemaeker et al16 conducted a study regarding optimization of Desflurane and Sevoflurane doses in morbidly obese patients using a inhalational bolus technique. In this study they concluded Immediate recovery was significantly faster in the Desflurane group. Similar results were obtained in my study. We found desflurane as satisfactory as sevoflurane for the maintenance of general anaesthesia as both the groups did not have any major respiratory and hemodynamic adverse event. Lerman et al17reported higher incidence (P < 0.006) of major adverse events, when extubation done in deep anaesthesia (15%) as compared to that in awake state (5%). We did not find any adverse event during emergence possibly because removed endotracheal tube in an awake state. Airway adverse effects were not noted among both groups. White PF Tang J et al18 concluded that Desflurane had high incidence of cough during recovery when compared to Sevoflurane. KLOCK PA Czeslick et al19 also 83 concluded that desflurane has more incidence of cough at 1MAC which was similar to our study. Emergence characteristics like time to regular breathing, time to awakening and time to extubation was faster with desflurane than sevoflurane when used for maintenance of general anaesthesia. As a result of the lower solubility of desflurane in blood and lean tissues, it is expected to find faster emergence with desflurane than sevoflurane.[55][56] Similar results were also obtained by Welborn et al. and Cohen et al. in their studies. Macario et al. in their meta-analysis also reported similar observations. This faster emergence with desflurane is really important in busy paediatric ambulatory setups.14,20,2 The occurrence of immediate postoperative nausea and vomiting (PONV) was noted for 30 minutes. No significant differences were detected in nausea and vomiting. Our study agreed with the Alex Macario et al study which also found that there was no significant occurrence of nausea and vomiting.14
CONCLUSION Thus from the above results and discussion we conclude that Desflurane had rapid emergence, recovery from anaesthesia and early discharge from PACU when compared with sevoflurane.
REFERENCES
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.