 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 10 Issue 2 -May 2019
Evaluation of the accuracy of finger-tip palpation of pilot balloon as a method to judge endo tracheal tube cuff pressure
Manohar Mane1, Prashant Lomate2*, J Paranjape3
1Associate professor, 2Associate professor, 3Professor And HOD, Department of Anesthesia, Bharati Vidyapeeth (Deemed to be University) Medical College and Hospital Sangli, Maharashtra, INDIA. Email: drprashantlomate@gmail.com
Abstract Aims and Objectives- To check the reliability of finger tip palpation of pilot balloon to judge the ETT cuff Pressure, to record the volume required to achieve the ETT cuff pressure of 25 cm H2O. Material and Methods- Total 100 patients of posted for surgery under general anesthesia were studied. After premedication, Induction done with inj. Propofol 2 mg/kg, inj. Succinylcholine 2 mg/kg. Female patients will be intubated with 7.0 no cuffed ETT, Male patients will be intubated with 8.0 no. cuffed ETT. ETT cuff will be inflated and cuff pressure was judged by palpation of pilot balloon method. Actual ETT cuff pressure was checked by ETT cuff manometer and recorded. Then the ETT cuff will be inflated by 1 ml incremental inflation of air and the actual air required toget the pressure of 25 cmH2O, and it will be again noted. Results– In 72 % cases ETT cuff pressure was above 30 cm H2O, in 18 % cases cuff pressure was in the recommended range (20-30 cm H2O), in 10% cases it was below 20 cm H2O Conclusion– ETT cuff pressure measurement using ETT cuff manometer should be highly recommended as routine method to inflate ETT cuff. Key Word: ETT cuff manometer, ETT cuff pressure, Air
INTRODUCTION Endotracheal intubation is the most reliable method of securing the airway. After intubation the ETT cuff is inflated to get effective seal between the ETT and Trachea. Maintaining proper peritubal seal is important to prevent aspiration and for preventing leaking of gases around the ETT during ventilation.1 At the same time it should be confirmed that the pressure is not very high as it may compromise the blood supply of tracheal mucosa. Many a times the cuff pressure is judged by the palpation of pressure in the pilot balloon of the ETT with fingers, and it is not monitored by proper instrument. The ideal ETT cuff pressure to be maintained is 20 – 30 cm H2O.1,2,3,4 Higher pressure can lead to various side effects like post-operative hoarseness of voice, tracheitis, tracheal stricture and may lead to trachea oesophageal fistula5,6,7. If the pressure is low it may lead to the aspiration of oral secretions leading to pneumonia. ETT cuff manometer is the instrument used to monitor the actual ETT cuff pressure8,9. In the present study, we want to evaluate the accuracy of conventional method of checking ETT cuff pressure by counterchecking it by using instrument i.e. ETT cuff manometer.
MATERIAL AND METHODS Ethical committee approval taken. Total 100 patients, of age 18-65 years posted for surgery under General Anaesthesia were included in the study. Informed written consent obtained. In operation theatre monitors were applied, all patients were premedicated with inj. Midazolam 1.5 gm iv, inj. Ondansetron 4 mg iv, inj. Pentazocine 30 mg iv. Induction was done with inj. Propofol 2 mg/kg, inj. Succinylcholine 2 mg/kg. Female patients were intubated with 7.0 no cuffed ETT, Male patients were intubated with 8.0 no. cuffed ETT, by a consultant anaesthesiologist and ETT cuff was inflated with air and cuff pressure was judged by palpation of pilot balloon method. Once the air entry is checked, the actual ETT cuff pressure was checked by ETT cuff manometer and was recorded. Then all the air from the cuff was removed and the amount of volume of air with which the cuff was inflated was recorded. Then the ETT cuff will be inflated by 1 ml incremental inflation of air and the actual air required to get the pressure of 25 cmH2O, and it will be again noted.
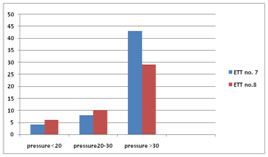
RESULTS Total 100 patients were studied. 55 were females and 45 were males. The mean age of patients were 46 years. EndoTracheal Tube cuff pressures were more than 30 cm of H2O in 72 cases (72%), average cuff pressure was 53.8 cm H2O. In 12 cases the pressure was above 100 cm H2O, ETT cuff pressure was on higher side in females as compared to males. In 18 cases (18 %) the cuff pressure was between 20-30 cm H2O i.e. in the recommended range. In remaining 10 cases (10 %) ETT cuff pressure was below 20 cmH2O.
Table 1: ETT size and ETT cuff pressure (cm H2O)groups
P<0.005 In patients in which 7 no ETT was used, in which the cuff pressure was on higher side, the average volume of air used to inflate the cuff were 4.7 ml .while in patients in which 8 no. ETT was used, in which the cuff pressure was found on the higher side was 6.6 ml.
Table 2: Average volume of air used
The average volume of air required to inflate the ETT cuff get 25 cm H2O was 3.45 ± 0.44 ml for 7 no. ETT cuff. While the volume of air required to inflate the ETT cuff of 8.0 no ETT, to get pressure of 25 cm of H2O was 4.5 ± 0.89ml.
Table 3: Average volume of air to get ETT cuff pressure of 25 cm H2O
DISCUSSION Endotracheal tube is used in operation theatre by anesthesiologist to provide general anesthesia, to control ventilation in a paralysed patient. Routinely the ETT cuff pressure is not measured using ETT cuff manometer. Most of the anaesthesiologist relay on palpation of pilot balloon of ETT for judging the adequacy of intra cuff pressure. Pressure exerted by ETT cuff on the mucosal surface of trachea is responsible for tracheal injury4,8,9. Intracuff pressure of more than 50 cm H2O totaly obstructs the blood flow to mucosa, and if the duration is for more than 15 minutes, it leads to tracheal epithelial injury. Conventional methods like palpation of pilot balloon by fingers, or loos of audible leak are not guaranteed methods and correlates poorly with actual intracuff pressure. most of the times it is on the higher side (i.e. >50 cm of H2O)such a high pressure leads to complications like sore throat, dysphagia cough in early post operative period. In our study the highest pressure recorded was 120 cm H2O, in this case the cuff was inflated with 10 ml of air. Mueen ullah Khan et al, studied the intracuff pressure using conventional method and rechecked the pressure again using instrumental method1. They used two different syringes 10 ml and 20 ml, to inflate the ETT cuff.in both the groups ETT cuff pressure was more than 30 cm H2O in 69% cases. This correlates to our study results. They concluded that conventional methods are unreliable. L Gilliland, H Perrie and J Scribante studied the ETT cuff pressure in two different hospitals. They found thatthe mean ETT cuff pressure was 47.5 cm H2O (range 10 -120 cm H2O). ETT cuff pressure was more than 30 cm H2O in 64.58 % cases in their study. Parvez Sultan et al, in their review article concluded that though ETT cuff pressure is not a major contributing factor for long term morbidity but there is clearly an inability among clinicians to adequately and reliability inflate the ETT cuff to the desired level. In our study, we also studied the average volume of air with which the cuff was inflated in conventional method, it was about 4.7 in 7.0 no ETT, while 6.6 ml in 8.0 no ETT. Sengupta et al mentioned in their study that the average volume of air to get the pressure between 20 -30 cm H2O was 2-4 ml irrespective of tube size for same type of tube. In our study we found the average air required to get the pressure of 25 cm H2O was 3.45 ml for 7.0 no ETT and 4.5 ml for 8.0 no ETT. Harm et al, in their study suggested the use of instrumental method to avoid inappropriately high intra cuff pressure. they also suggested use of 5 ml syringe to inflate the ETT cuff.
CONCLUSION From the above study it is concluded that use of aneroid manometer is highly recommended to check the ETT cuff pressure. Volume of air used to inflate the ETT cuff should be 3-4.5 ml.
REFERENCES
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.