 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 10 Issue 2 -May 2019
Retrospective study on various trauma cases in our emergency trauma care centre
G R Rajashree1*, Samuel Prabakaran2, V Rajesh3
{1Professor & HOD Trauma care, 2Chief Neuro-anaesthesiology, Department of Anesthesiology} {3CMO} RGGGH, MMC, Chennai, Tamil Nadu, INDIA. Email: dr.rajashree@hotmail.com
Abstract Background: In our trauma care centre we receive around 100-200 cases per day and 1000-2000 cases per month ranging from Polytrauma, Faciomaxillary injury, Both bone fracture Upper limb, Lower limb, Vascular trauma, Abdominal injuries of patients of variable age groups. Road traffic accidents is a major cause of death in India, despite preventive measures taken by the Government for personal protection like helmet for rider and the pillion rider, seat belt and airbags. Methods: Retrospective data was obtained from trauma registries from January 2018 to December 2018 regarding trauma related admissions, treatment, death and pre-hospital assistance. The collected data was analysed and the study on reduction of mortality was done. Key Words: Trauma, Injury, Death.
INTRODUCTION A Road Traffic Accident (RTA) can be defined as, ‘An event that occurs on a way or street open to public traffic; resulting in one or more persons being injured or killed, where at least one moving vehicle is involved. RTA is a collision between vehicles; between vehicles and pedestrians; between vehicles and animals; or between vehicles and geographical or architectural obstacles.’ Road traffic accidents are a human tragedy. They involve high human suffering and socioeconomic costs in terms of premature deaths, injuries, loss of productivity, and so on. If no action is taken, road traffic crashes are predicted to result in the deaths of around 1.9 million people annually by 2020. Hence the goal of the United Nations’ Decade of Action for Road Safety 2011- 2020 is to save five million lives. According to the World Health Organization (WHO), road traffic injuries are the sixth leading cause of death in India with a greater share of hospitalization, deaths, disabilities and socio-economic losses in the young and middle-aged population. Road traffic injuries also place a huge burden on the health sector in terms of pre-hospital and acute care and rehabilitation.
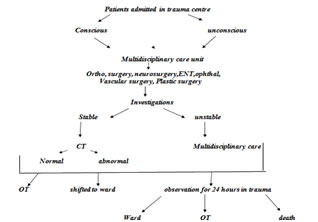
MATERIAL AND METHODS The study was conducted in Rajiv Gandhi Government General hospital, Madras Medical College, Chennai. After obtaining approval from the Institutional Ethics Committee, retrospective data was obtained from trauma registers. Details of various trauma cases like Polytrauma, fracture mandible/zygomatic process, long bone fracture upper limb, long bone fracture lower limb, lacerated wound, unconscious patients with severe head injury, chest injury, abdominal injury, stab injury, injury by assault, cut throat injury, spine injury with or without neurologic manifestations, ophthalmic injuries and vascular injuries was noted for a period of 12 months from January 2018 to December 2018. Paediatric cases, patients brought dead and unknown patients who were unconscious were excluded. Depending on the vitals and investigations, patients were considered either stable or unstable. Multidisciplinary care was given to each patient. Stable patients were either shifted to the operation theatre or to the ward for conservative or medical management. Unstable patients were observed for 24 hours in trauma ward and then were either shifted to the operation theatre or the ward or succumbed to their injuries. Collected Data was analysed using SPSS analysis software 23.0 Version which includes tests like Shapiro Wilk’s test, Unpaired sample t-test, ANOVA and Chi-Square test was used.
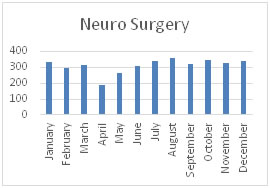
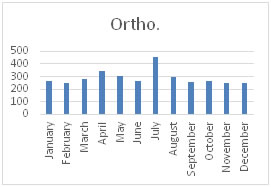
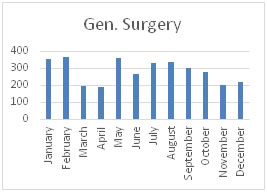
RESULTS Data for a total of 11029 patients was collected. July recorded the most cases with 1157 cases. April recorded the least cases with 734 cases. Neurosurgery had the most cases with 3729 cases with an average of 310.75 cases every month. Neuro Surgery recorded a total of 3729 cases with an average of 310.75 cases every month. August recorded the most Neuro Surgery cases with 356 cases. April recorded the least cases with 186 cases. Orthopaedics recorded the second most cases after Neurosurgery with 3482 cases with an average of 290.16 cases every month. July recorded the most Orthopaedics cases with 456 cases. February recorded the least cases with 247 cases. General Surgery recorded a total of 3409 cases in the 12 months with an average of 284.08 cases every month. February recorded the most General Surgery cases with 368 cases. April recorded the least cases with 191 cases.
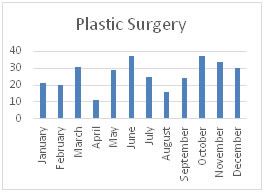
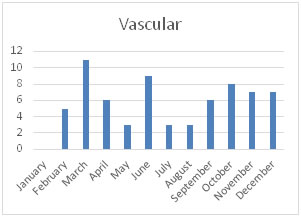
Plastic Surgery recorded a total of 315 cases with an average of 26.25 cases every month. June and October recorded the most Plastic Surgery cases with 37 cases each. April recorded the least cases with 11 cases. Vascular Surgery recorded a total of 68 cases with an average of 5.66 cases every month. March recorded the most Vascular Surgery cases with 11 cases. January recorded the least cases with 0 cases.
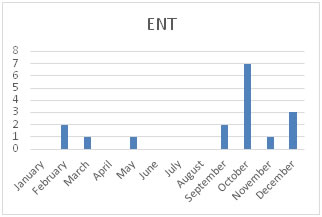
ENT recorded a total of 17 cases with an average of 1.41 cases every month. October recorded the most ENT cases with 7 cases. January, April, June, July and August recorded the least cases with 0 cases.OMFS recorded a total of 9 cases with an average of 0.75 cases every month. February and June recorded the most OMFS cases with 2 cases. January, April, May, September and December recorded the least cases with 0 cases. January recorded the highest death rate of 8.27% with October recording the lowest of 2.61% with October, November and December all recording death rates < 3%. 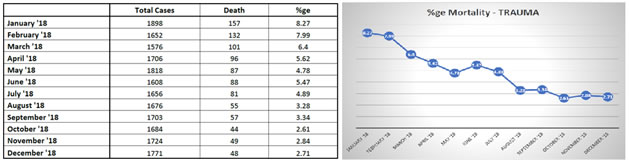
DISCUSSION The idea of Trauma care initiative in our setup was born with the thought of providing immediate aid to the acute trauma patients without any delay. The provision of efficient and immediate care and monitoring were the important points of the program. Neurosurgery recorded most number of cases in line with the fact that road traffic injuries are the sixth leading cause of death in India with a greater share of hospitalization, deaths, disabilities and socio-economic losses in the young and middle-aged population, as recorded by WHO. Outcome of any program is always dependent on the team which consists of the doctors of all specialties, the trained staff nurses, the paramedics and the availability of all the required drugs, monitors and gadgets. Awareness and streamlining of any trauma care centre will make it easy to provide immediate multispecialty attention, care and recovery of the patient.
CONCLUSION In our trauma centre, Neurosurgery recorded the most cases, indicating the high proportion of head and spine injuries, followed by Orthopaedics and General surgery. Introduction of the Trauma care initiative and the triage zones has been a milestone and has led to the improvement of the mortality from 8.27% in January 2018 to consistently record less than 3% by the end of December 2018.
|
|

 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.