 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 10 Issue 2 -May 2019
Incidence of complications after prophylactic phenylephrine and placebo in elective urological surgeries
Meghna Maheshwari1, Kashish Ahuja2*
1Assistant Professor, Department of Anesthesiology, Sri Aurobindo medical college and PG institute, Indore, INDIA. 2Professor and HOD, Department of Anesthesiology, Bombay hospital, Indor, INDIA. Email: cara_4999@yahoo.com
Abstract Background: Spinal anesthesia is commonly practiced neuraxial anesthesia for various surgeries including gynecological, obstetrics, urological, orthopedics, etc. The most common impediments to the effective use of neuraxial blocks are the predictable decreases in arterial blood pressure and heart rate through the accompanying sympathectomy with its attendant vasodilation and blockade of cardioaccelerator fibers. Maintaining arterial blood pressure and heart rate at normal values during these blocks often requires the administration of vasoactive drugs and intravenous fluids. The most common complication of this anesthetic technique is hypotension, with a particularly frequent incidence in the elderly. Aim and objectives: To study the Incidence of complications after prophylactic phenylephrine and Placebo in Elective Urological Surgeries for prevention of hypotension. Materials and method: The present randomized controlled, double blind study was conducted in the department of anaesthesia of tertiary care institute to study complications after prophylactic phenylephrine and Placebo used for prevention of post Sub Arachnoid Block hypotensive response in patients undergoing elective urological surgeries under Sub Arachnoid Block” Total 60 patients were enrolled in the present study and were divided in to two groups conationg 30 patients each. A computer generated randomized plan was made, which placed patients randomly in the two groups. Group P (Phenylephrine group) and Group C (Control group). The group P Patients received phenylephrine(2mg i.m.) preoperatively. After preloading pulse rate, systolic and diastolic blood pressure were recorded. The same parameters were recorded at following intervals; just prior to administration of inj phenylephrine (baseline), after subarachnoid block, every 2 min for 15 min and thereafter every 5 min till the end of the surgery. The collected data was recorded in excel sheet and was analysed with appropriate tests. A value of P<0.05 was considered statistically significant. Results: Both the groups were similar in age, ASA status, sex distribution and baseline hemodynamic variables. Hypotension was observed in 3.33% patients in group P while in 43.33% patients in group C and the difference observed statistically significant. Other than hypotension nausea was the other most common complication observed in group C patients. The percentage decreases in HR in the two groups were not significantly different. The lowest HR value in all groups was <50 bpm, and equal percent of patient in each group developed bradycardia and required medication after spinal anesthesia. Only one patient in the group P required nicardipine because of hypertension after the study medication. No patient in the other group developed hypertension. Conclusion: Based on the findings of the present study, we conclude that use of phenylephrine before sub arachnoid block causes less incidence of post sub arachnoid block hypotension and complications associated with it like nayusea, vomiting. Key Word: Intramuscular phenylephrine, hypotension, spinal anaesthesia, complications
INTRODUCTION Spinal anaesthesia is commonly practiced neuraxial anesthesia for various surgeries including gynaecological, obstetrics, urological, orthopaedics, etc. The most common impediments to the effective use of neuraxial blocks are the predictable decreases in arterial blood pressure and heart rate through the accompanying sympathectomy with its attendant vasodilation and blockade of cardio accelerator fibers. Maintaining arterial blood pressure and heart rate at normal values during these blocks often requires the administration of vasoactive drugs and intravenous fluids.1The most common complication of this anaesthetic technique is hypotension2,3, with a particularly frequent incidence in the elderly.4-6 Using bupivacaine0.5%, spinal anaesthesia can provide appropriate regional anesthesia for patients with hip fracture.7 Cardiovascular effects of neuraxial block are similar to the intravenous (IV) use of alpha 1 and beta blockers and their effects on the cardiovascular system which can be emerged as decline in heart rate and arterial blood pressure.8 In old patients and those who suffer from heart diseases, the rate of peripheral vascular resistance after spinal anesthesia may be reduced up to 25%, and the amount of cardiac output may drop to 10% as well.9 Ephedrine is a noncatecholamines sympathomimetic drug, which is usually used IV. Ephedrine increases blood pressure and heart rate.10 Phenylephrine is an alpha‑1 receptors agonist that is used when peripheral vasoconstriction is needed and heart records are acceptable and appropriate similar to what occurs in spinal anesthesia. The cardiovascular effects of neuraxial blocks are similar in some ways to the combined use of IV alpha 1‑ and beta‑adrenergic blockers: Decreased heart rate and arterial blood pressure. When phenylephrine is IV used, it is a drug with rapid onset and short duration of action (5–10 min).11 In previous studies, the effect of phenylephrine and ephedrine has been used to prevent hypotension in spinal anaesthesia and different results have been taken. Magalhães et al. in 2009 compared the efficacy of ephedrine and phenylephrine in the prevention and treatment of maternal hypotension during spinal block. Two groups to receive IV prophylactic ephedrine (Group E, n = 30, dose = 10 mg) or phenylephrine (Group P, n = 30, dose = 80 μg). They found that ephedrine was more effective than phenylephrine in the prevention of hypotension.12 Nishikawa et al. in 2002 investigated prophylactic intra muscular small dose phenylephrine on spinal anaesthesiainduced hypotensive during surgical repair of hip fracture in the elderly.13 In this study, the effect of preventive singledose of IM phenylephrine to prevent hypotension after spinal anaesthesia was studied along with its safety and associated complications was studied. AIM AND OBJECTIVES To study the Incidence of complications after prophylactic phenylephrine and Placebo in Elective Urological Surgeries for prevention of hypotension.
MATERIALS AND METHOD The present randomized controlled, double blind study was conducted in the department of anesthesia of thertairy care institute to study complications after prophylactic phenylephrine and Placebo used for prevention of post Sub Arachnoid Block hypotensive response in patients undergoing elective urological surgeries under Sub Arachnoid Block”. Following criteria was used to select the study subjects.
With reference to above mentioned selection criteria total 60 patients were enrolled in the present study and were divided in to two groups conationg 30 patients each.A computer generated randomized plan was made, which placed patients randomly in the two groups.
A thorough pre-anesthetic checkup of all the patients was carried out and necessary investigations were performed preoperatively. Details of the procedure were explained to all the patients and written consent was obtained. This computer generated randomization sheet was handed over to the pharmacist so as to make and supply syringes of the drug and placebo according to the patient number in the sheet. Observations were made by the anesthesiologist conducting the case. After the data collection of 60th patient, proforma case sheets were segregated in two groups – group P and group C- according to the randomization sheet. Anesthesia Technique: A vein was cannulated with a wide bore intravenous cannula; Ringer lactate solution 500ml was infused as preload. The patient was monitored with non-invasive BP, ECG monitor and pulse oximeter. After pre loading patient was given an IM dose of 2mg phenylephrine, 15 min prior to administration of subarachnoid block. After careful antiseptic preparation and draping, subarachnoid block was given in sitting position. A Quincke spinal needle 26gauge was passed into the subarachnoid space at L2-3 or L3-4. After observing free flow of cerebrospinal fluid, inj bupivacaine 0.5% hyperbaric 2.5 ml plus 20mcg of inj Fentanyl was given through the spinal needle. The patient was made supine. Interventions and Observations: After preloading pulse rate, systolic and diastolic blood pressure were recorded. The same parameters were recorded at following intervals:
Whenever hypotension i.e. a fall in systolic blood pressure of 20% from the base line value occurred, intermittent IV bolus of 3mg ephedrine was given as rescue drug. The bradycardia i.e. a pulse rate of 50/min or less was treated by inj Atropine 0.3 mg IV. Hypertension i.e. rise in systolic B.P. of 20% from the baseline value was treated with s/l depin administration. The maximum level of sensory block was assessed by pinprick method 5 min after the SAB. All the complications observed in the study were recorded and were compared in the both the groups. The collected data was recorded in excel sheet and was analysed with appropriate tests. A value of P<0.05 was considered statistically significant.
RESULTS Table 1: Distribution of patients according to baseline data
In the present study total 30 patients were enrolled in each group. The mean age of patients in group P and group C was 51.26±11.01 yrs and 50.70±10.99 yrs respectively. All the patients were of ASA grade I and II with 15 cases each in both the groups. The baseline heart rate in group P and group C was 76.06±9.13 bpm and 85±9.50 bpm respectively. The mean systolic blood pressure was 120.6±11.32 mm Hg and 120.73±12.23 mm Hg in group P and group C respectively. The average Sensory dermatomal level among both the groups was T9 with range from T8 to T10. Thus both the groups were similar in age, ASA status, sex distribution and baseline hemodynamic variables. Table 2: Incidence of hypotension in both the study groups
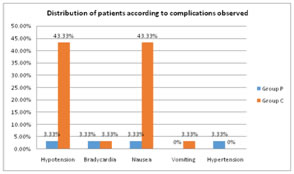
X2 =13.14, df=2, p<0.01 (highly significant) Hypotension was observed in 3.33% patients in group P while in 43.33% patients in group C and the difference observed statistically significant. Table 3: Distribution of patients according to complications observed.
It was seen that other than hypotension nausea was the other most common complication observed in group C patients. The percentage decreases in HR in the two groups were not significantly different. The lowest HR value in all groups was <50 bpm, and equal percent of patient in each group developed bradycardia and required medication after spinal anesthesia. Only one patient in the group P required nicardipine because of hypertension after the study medication. No patient in the other group developed hypertension.
DISCUSSION The present study was conducted in the department of Anesthesia with the aim to study the complications after prophylactic phenylephrine and Placebo in Elective Urological Surgeries. In the present study total 30 patients were enrolled in each group. The mean age of patients in group P and group C was 51.26±11.01 yrs and 50.70±10.99 yrs respectively. All the patients were of ASA grade I and II with 15 cases each in both the groups. The baseline heart rate in group P and group C was 76.06±9.13 bpm and 85±9.50 bpm respectively. The mean systolic blood pressure was 120.6±11.32 mm Hg and 120.73±12.23 mm Hg in group P and group C respectively. The average Sensory dermatomal level among both the groups was T9 with range from T8 to T10. Thus both the groups were similar in age, ASA status, sex distribution and baseline hemodynamic variables. Similar findings were also reported by Abbasivash R14and Somayaji AS,15 in their studies. Hypotension was observed in 3.33% pateinst in group P while in 43.33% patients in group C and the difference observed statistically significant.Vasopressors are often used for counteracting hypotension following spinal anesthesia. Sahu et al. have reported that maternal hypotension during SA for caesarean section in nearly 85% of patients.16 This high incidence could be due to factors such as the amount of drug (local anaesthetic) injected, sympathetic blockade, and compression of the inferior vena cava by the gravid uterus compromising the venous return.17Somayaji AS,15 also found phenylephrine to be better for the prevention of hypotension. It was seen that other than hypotension nausea was the other most common complication observed in group C patients. The percentage decreases in HR in the two groups were not significantly different. The lowest HR value in all groups was <50 bpm, and equal percent of patient in each group developed bradycardia and required medication after spinal anesthesia. Only one patient in the group P required nicardipine because of hypertension after the study medication. No patient in the other group developed hypertension. Intramuscular (IM) administration of vasopressors has been tried in the past with good outcomes,18,19 but there have been no studies comparing IM routes for different vasopressors. Time for the onset of action after IV administration is 15–30 s, whereas it is 10–20 min after IM administration.20 This time gap can buy enough time for slow and gradual action of the drug, thus providing better hemodynamic stability during the intraoperative period with lesser side effects in patients.18 Thus Intramuscular (IM) administration of phenylephrine reduces the proportion of complication.
CONCLUSION Based on the findings of the present study, we conclude that use of phenylephrine before sub arachnoid block causes less incidence of post sub arachnoid block hypotension and complications associated with it like nayusea, vomiting.
REFERENCES
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.