 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 10 Issue 2 -May 2019
Comparison of haemodynamic changes during laproscopic surgery and postoperative analgesia while using fentanyl and butorphanol as a premedication
Vishal Shrimali1, Bhavin Patel2*
1Assistant Professor, 2Senior Resident, Department of Anesthesiology, GMERS Medical College, Gotri, Vadodara-390021, INDIA.
Abstract Back ground and Aim: Laproscopy surgery has advantages like minimal tissue trauma, reduced post operative complication and early recovery to normal activity. Laproscopy requires pneumoperitoneum which causes various cardiovascular and respiratory derangements especially tachycardia, hypertension, increased central venous pressure, direct myocardial depression. There are various pharmacological agents used during laproscopic surgery for haemodynamic stability like B-blockers, nitroglycerine, alpha2-agonist (dexmedetomidine, clonidine), opioids e.g(fentanyl, sufentanyl, morphine, butorphanol). We carried out the present study to compare the effect of Butorphanol and Fentanyl as a premedication on haemodynamic changes during laproscopic cholecystectomy surgeries and postoperative analgesia. Methodology: Fifty patients posted for laproscopis cholecystectomy surgeries of ASA grade I and II, 20-40 years age of either sex were selected for this study. They were randomly divided in two groups of 25. Group B Received Inj. Butorphanol 40 mcg/kg and Group F received Inj.Fentanyl 2 mcg/kg as a premedication. Haemodynamic parameter(pulse rate, systolic blood pressure, diastolic blood pressure,etco2) was measured during surgery. Postoperative pain was assessed by VAS score and analgesia given only when the score was ≥5. Results: It was Observed that much more stable haemodynamic parameters seen during surgeries in Group B as compared to Group F. Requirement of First dose of analgesic was significantly longer in group B[3hrs] than group F[30 min]. Conclusion: This study concluded that Butorphanol is a useful alternative to Fentanyl as a premedication because of its ability to produce stable haemodynamic changes during surgeries and longer postoperative analgesia. Key Word: Butorphanol, Fentanyl, Laproscopy.
INTRODUCTION laproscopic surgery also called as minimal invasive surgery, in which operation were performed through small incisions. laproscopically examining the peritoneal cavity was first attempted in 1901 by George kelling who called this examining procedure "celioscoy". First laproscopic surgery on human was done in 1987 by French doctor mouret. laproscopy has been promoted aggressively as gentle surgery and has advantages like minimal tissue trauma, reduced post-operative complication and early recovery to normal activity. Laproscopy requires pneumoperitoneum for good visualization.CO2 is most commonly gas used, other gases used are air, helium, nitrogen. Pneumoperitoneum causes various cardiovascular and respiratory derangements. On cardiovascular system it causes tachycardia, hypertension, increased central venous pressure, direct myocardial depression and increase in after load-catecholamines, vasopressin, renin angiotensin activity. There are various pharmacological agents used during laproscopic surgery for haemodynamic stability like B-blockers, nitroglycerine, alpha2-agonist(dexmedetomidine, clonidine), opioids e.g(fentanyl, sufentanyl, morphine, butorphanol). Narcotic drugs blunts the effect of haemodynamic changes which is created by pneumoperitoneum during laproscopic surgery. Narcotic analgesia is widely used as an adjuvant to general anaesthesia. This acts to smoothen the intra operative course, decreases requirements of other anaesthetic agent, smoothen recovery and minimize postoperative pain. Butorphanol is synthetically derived opioid having agonist-antagonist action on its receptors. It is agonist at k-receptor and partial antagonist at u-receptor. It causes decrease in heart rate and blood pressure. It also produces sedation by its action on k-receptor and analgesia action by acting on k-receptor and u-receptor. Fentanyl is synthetic opioid. It is u-receptor agonist, it acts on u -receptor at supra-spinal sites and produces analgesia. Fentanyl is a cardio-stable drug. Both of these drugs causes decrease in pulse rate and blood pressure but the effect is more intense in Butorphanol drug. Aim of our study were to compare Butorphanol and Fentanyl as a premedication in laproscopic surgery in terms of haemodynamic changes (pulse and Blood pressure, Etco2) and postoperative sedation and analgesia.
MATERIALS AND METHOD This prospective randomised double blind study was conducted after approval from our institution (gmers medical college, Baroda) and written informed consent from the patients. For this study 50 adult patients undergoing, laproscopic cholecystectomy surgeries of age group 20-60 years of either sex, ASA I andII were selected. Exclusion criteria were age <20 years and >40 years, ASA III andIV, history of drug allergy, pregnant or lactating women, patients having any cardiac disease, patients having upper respiratory tract infection. All the patients were thoroughly investigated. All the patients received Tab. Diazepam(10 mg) and Tab. Rantac (150 mg) orally on previous night of surgery. Patients were kept nil by mouth for 8 hours before surgery. On the day of surgery after taking written informed consent, patients were premedicated with inj. Glycopyrrolate 0.2 mg IM 30 minutes before induction of anaesthesia and inj. Ranitidine 50 mg and inj. Ondansetron 4 mg were given IV. Monitors were attached and all baseline parameters pulse rate, blood pressure,spo2, after intubation Etco2 was also measured. Four minutes before induction of anaesthesia, patients divided into two groups. Group B received inj. Butorphanol 40 mcg/kg intravenously while Grouop F received inj. Fentanyl 2 mcg/kg intravenously as premedication. Patients were preoxygenated for 3 minute with 100% o2 through bain's circuit. All the patients were induced with inj. propofol 2.5 -3 mg/kg IV till loss of eye reflex, inj. succinyl choline 1.5 -2 mg/kg IV followed by tracheal intubation. Anaesthesia was maintained with controlled ventilation with 02and N2o (50:50), isoflurane(0.2 -1.5%) and intermittent inj. vecuronium bromide (0.02 mg/kg) IV. Intra-abdominal pressure was kept between 11-15 mm of hg. Throughout course of anaesthesia patients were monitored for haemodynamic parameters pulse, systolic blood pressure, diastolic blood pressure, Etco2, and Spo2.After giving drug, after intubation, every 3 minute after intubation till 20 minutes. Before pneumoperitonium, 15 min interval till 1 hour of pneumoperitonium, after release of CO2, after extubation. After completion of surgery, patients were reversed with inj. Neostigmine50 mcg/kg IV and inj. Glycopyrrolate 10mcg/kg IV. In the postoperative period, each patient was monitored for haemodynamic parameters, sedation score, VAS score for pain relief and post-operative complications like nausea, vomiting, rashes, excitement, dizziness, urinary retention, respiratory depression, pruritus. Table1: Sedation score
RESULTS Study of adult patients of either sex, ASA I II, undergoing laproscopic cholecystectomy. They were divided randomly into two groups, Group B received inj. Butorphanol 40 mcg/kg IV and Group F received inj. Fentanyl 2 mcg/kg IV. All parameters and variables were subjected to statistical analysis using unpaired t-test and chi square test and p-value(>0.05 insignificant, <0.001 highly significant).As shown in table:2 ,there were no difference in age ,sex, weight, ASA grading and duration of surgery in both groups. Table 2: Demographic Data:
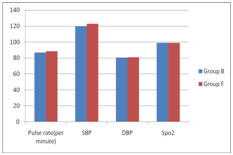
Table 3: Pre-operative vital parameters
The preoperative value of pulse, systolic blood pressure, diastolic pressure in both the groups were shown in table:3, suggestive that both groups were comparable.
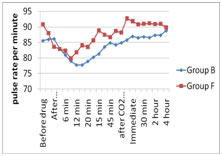
Table 4: Changes in pulse rate
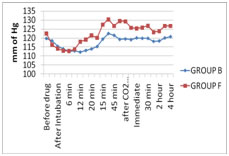
As shown in table; 4 comparing both groups, no significant changes in pulse rate were seen till 9 min after intubation, however significant difference in pulse rate was started at 12 min after intubation and persisted till 2nd hour of postoperative period. No statistical difference was found between both the groups at 3rd and 4th hour of postoperative period. Table 5: Systolic blood pressure
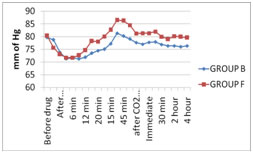
Table 6: Diastolic Blood pressure changes
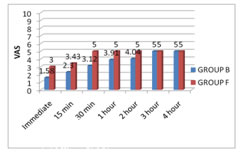
On comparing both the groups for systolic blood pressure in table:5, no significant difference was found till 9 min after intubation, than onwards significant changes were noted till 4th hour of postoperative period. As shown in table:6 no changes in diastolic blood pressure were noted till 9 min after intubation. The statistical difference in diastolic blood pressure started at 12 min after intubation and persisted till 4th hour of postoperative period. There were no significant changes in the etco2 in both groups. Patients of group F were started having pain at 30 min after extubation in comparison to Group B patients having pain after 3 hour and comparison of both the groups was found to be significant till 4th hour of postoperative period. Rescue analgesia was given in form of inj. Diclofenac sodium when patient VAS score ≥5/10, this was taken as a end point of pain relief. Table 7: Visual Analogue scale of pain(VAS):
In postoperative period in Group B sedation remained for longer period for about 3 hours, while in Group F sedation remained for 30 min after extubation. Comparative study was found to be statistically highly significant (p<0.001) till 30 min after extubation, at 1st and 2nd hour of postoperative period difference was found to be statistically significant (p<0.05).No significant change in sedation score was seen at 3rd and 4th hour of postoperative period. Table 8: Sedation score
There were complications like nausea, vomiting, and rashes in few of the cases. The incidence of vomiting(4%) and nausea(8%) were more in case of Group B compared to Group F which was found to have vomiting(12%) and nausea(12%).There was incidence of rash (4%) in case of Group F ,no such incidence of rash was found in Group B.
DISCUSSION Now a days laproscopic surgery has replaced many of the open surgeries because of its advantage like fast recovery, less incidence of complication and relatively less painfull. There are various haemodynamic, respiratory and stress response changes in laproscopic surgery due to creation of pneumoperitoneum. In balanced anaesthesia ideal opioid would permit rapid titration to the effect, successfully prevent unwanted responses to various stimuli, require little supplementation, does not depress cardiovascular function, permit the return of adequate spontaneous ventilation in timely manner and produce residual if not complete postoperative analgesia with minimal side effects. Butorphanol, a synthetic opioid derivative is a mixed agonist-antagonist with analgesic potency greater than morphine and pethidine. Butorphanoland and its metabolites are agonist at kappa receptors and mixed agonist-antagonist at mu receptors. It has also sedative action. Butorphnol unlike morphine exhibits a ceiling effect on respiratory depression. Fentanyl is also cardiostable and have analgesic action. Fentanyl acts on mu receptors at supra-spinal sites. Both the groups of drug have haemodynamic stability, analgesic action, sedation and decreases the requirements of other anaesthetic drugs and are available at low cost, so we have chosen Butorphanol and Fentanyl to study haemodynamic changes and analgesic action in both the groups. Mean age in group B was 38.5±8.40 and group F was 43.75±10.94 years and both the groups were comparable9,17. Mean weight in group B was 51.87±4.57kg and in group F was 50.96±5.72 kg, observation were found to be comparable9,17 .The duration of surgery in group B was found out to be 111.17±9.07 min and in group F was 112.87±9.48,both the groups were comparable, while in other studies duration of surgery were 90 min and 50 min which is not in consonance with our study7,9,17.As shown in graphs it was found that pre-operative vital parameters ( pulse rate, systolic blood presuure, diastolic blood pressure,spo2) were comparable in both groups.
The changes in the pulse rate were comparable in both the groups. As shown in the graphs, there were very minor changes in pulse rate in both the groups till 12 min after intubation. Comparing the mean pulse rate in both groups from 12 min after intubation till 2nd hour of postoperative period was found to be significant. There was no significant difference in the pulse rate was noted in both groups at 3rd and 4th hour of postoperative period. Comparing both the groups fall in pulse rate in group B was more in comparison to group F throughout perioperative period. The deviation in pulse rate in both groups was not to the extent of bradycardia or tachycardia (≤20% of preoperative value). R.K.Verma et al found suppression of sympathetic responses to laryngoscopy and intubation was better with butorphanol than fentanyl, which was in consonance with our study. Bevely K. Philip et al noted that intraoperatively patients who received butorphanol demonstrated lower pulse rate before, after intubation and perioperative period. Pandit et al studied that only statistically significant changes occur 2 min after tracheal intubation in fentanyl group when pulse rate was significantly higher than preoperative baseline values, while such rise in pulse rate was noted in butorphanol group. Mean systolic blood pressure were comparable in both the groups. As shown in the graphs, there were very minor changes in the systolic blood pressure in both the groups till 9 min after incubation. Than after comparing the mean systolic blood pressure in both the groups 12 min after intubation, till 4th hour of postoperative period was found out to be significant. There were no incidence of hypertension and hypotension in both groups. Comparing both the group, in group F there was rise in systolic blood pressure more after creation of pneumoperitoneum till postoperative period than in comparison to group B. Beverly K. Philip et al found in their study that there were no significant changes in systolic blood pressure, our study was in consonance with their study. Both the groups were comparable with respect to diastolic blood pressure. There were significant changes noted on comparing both the groups from 9 min after intubation till 4th hour of post-operative period. Fall in diastolic blood pressure was seen more in case of butorphanol group than in comparison to fentanyl group. There were no incidence of hypotension or hypertension in both the groups. There were no significant changes in the end tidal volume of CO2 were noted in both groups. The amount of inhalation agent used in group F(1.8%-2%) was more in comparison to group B(1.3%-1.5%).17. In case of group F, in order to control blood pressure we used to start Propofol drip in 12% of cases when blood pressure was not controlled even after inhalation concentration beyond 2% and the rise in pulse rate and blood pressure were >20% of the base line values. As per observation sedation in group F was found upto 1 hour and in group B was upto 3 hours in post-operative period. So it was found that postoperatively sedation was more in case of group B than in comparison to group F. R.K.Verma et al found that the emergence time, recovery time and post operative sedation was more in butorphanol group than in the fentanyl group. Beverly K.Philip et al used butorphanol(20 mcg/kg) and fentanyl (1mcg/kg) as premedication, postoperative sedation was observed more in butorphanol group during first 45 min of recovery. In other studies they observed post-operative sedation, amnesia, drowsiness, longer pain relief with butorphanol7,9,15,16,17. So our study is consistent with all above studies. As butorphanol is a strong kappa receptor agonist with weak mu receptors antagonist, it is associated with more sedation. Visual analogue scale(VAS) method is widely used accepted method for pain assessment9,13,15,17. On analysing postoperative pain relief on VAS, group B showed analgesia upto 3 hours as compared to group F showed pain relief upto 1 hour and difference was statistically significant(p<0.05). Hammad usmani et al in their study found out that time to first rescue analgesia was also significantly prolonged in butorphanol group as compared to fentanyl group. In other studies they observed longer pain relief in butorphanol group as compared to fentanyl groups9,10,11,14,15. On considering post-operative complication, both groups were comparable as far as incidence of nausea was 8%, vomiting 4% in group B as comparison to group F in which nausea 12%, vomiting 12% and rashes 4% were found. However PONV were easily treated with inj. Ondansetron 4 mg intravenously and rashes in group F were treated with inj. Chlorpheniramine maleate 5 mg intravenously CONCLUSION We concluded that butorphanol is better alternative to fentanyl as a premedication for use in laproscopic surgeries because of its ability to produce haemodynamic stability, prolong analgesia and less postoperative complication.
REFERENCES
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.