 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 10 Issue 3 -June2019
Intrathecal isobaric ropivacaine compared with hyperbaric bupivacaine for lower segment caesarean section
Madhu K R1, Suresh S B2*
1Assistant Professor,2Professor, Department of Anaesthesiology, Shridevi Snstitute of Medical Sciences and Research Hospital, NH-4, Bypass Road, Tumkur- 572106, INDIA. Email: hrbs2006@yahoo.co.in
Abstract Background: The aim of this study was to compare clinical efficacy and safety of isobaric ropivacaine and hyperbaric bupivacaine in spinal anaesthesia for elective cesarean section. Methods: A prospective, randomized study was performed in 100 patients with Term parturient measuring height of 155 to 165 cm with singleton pregnancy undergoing elective Caesarean section, randomly allocated in two groups after obtaining valid written informed/explained consent, group R (ropivacaine n=50), group B (bupivacaine n=50). Spinal anaesthesia was performed in left lateral position, with table being neutral position at the L3-L4 or L4-L5 levels and 2 ml of 0.75% isobaric ropivacaine or 0.5% hyperbaric bupivacaine was administered. Time for onset of sensory and motor block, maximum cephalad spread of sensory block, time for regression, time to request for rescue analgesia, total duration of motor block, quality of anaesthesia were assessed. Also influence of the blockade on the function of the cardiovascular and respiratory system, adverse events and requirement additional medications were recorded. All data was statistical analysed. Results: In our study, onset of sensory block at T8 was slightly prolonged with ropivacaine172.8 ± 82.7 sec compared to bupivacaine151 ± 88.30 sec, P= 0.012. Complete motor block was delayed with plain ropivacaine 498 ± 289.5sec, compared to bupivacaine, Group B- 249 ± 181.3 sec, P = 0.001. Motor block regressed faster with ropivacaine, 94.24 ± 17.58 min, compared to bupivacaine 210.62 ± 44.98 min, P = 0.001. Time of request of analgesia is comparable in both groups. Regression to L1 is shorter in case of ropivacaine 157.4 ± 34.52 min, in comparison with bupivacaine181.6 ± 43.72 min, P = 0.000 Haemodynamic parameters and respiratory function were similar in both groups. Both ropivacaine and bupivacaine produced favourable surgical conditions. There were no significant differences between the groups with respect to side-effects, and additional requirement of medication and the quality of the blockade. The scores of quality of anaesthesia assessed by surgeons was similar in both groups. Conclusion: 15mg 0.75% isobaric ropivacaine provides safe and equally effective spinal anaesthesia with reduced duration of motor block, compared to 10 mg 0.5 % hyperbaric bupivacaine for cesarean section. Both provide satisfactory analgesia and good surgical conditions. Key Word: Bupivacaine, Cesarean section, Ropivacaine, Spinal anaesthesia.
INTRODUCTION In India as per District level household survey 3 (DLHS) CS rate is 28.1% in private sector and 12% in public sector health facilities. This survey shows share of Cesarean deliveries in institutional births have increased in India, especially in private sector health facilities. And a steady increase by 1% each year is observed.1 Spinal anaesthesia is the most common method of anaesthesia for elective and emergency caesarean sections. The rapidity of spinal onset is especially useful in cases where delivery of the foetus must be expedited due to a compromised foetal state. Spinal anaesthesia, being easy technique hence become anaesthesia of choice for caesarean section world wide.2 Motor block beyond the duration of surgery during subarachnoid block is undesirable, particularly in ambulatory setting. Many local anesthetic agents have been used in spinal anesthesia. Ropivacaine is one among them, Ropivacaine (1-propyl-2”, 6”-pipecoloxylidide) is amino amide local anesthetic (LA) drug that chemically and pharmaco dynamically resembles bupivacaine. Ropivacaine is an enantiomer whose intrathecal administration has been investigated. introduced clinically in 1992, only isobaric ropivacaine is available in the market, glucose is usually added to make it hyperbaric solutions. Ropivacaine provides shorter duration of sensory and motor block than compared to bupivacaine, hence used in short duration surgeries and day-case setting. Many studies have compared the clinical efficacy and side effects on identical doses of intrathecal ropivacaine and bupivacaine in spinal anaesthesia. Very few studies have been performed comparing intrathecal use of equal volume of isobaric ropivacaine and bupivacaine and studying there hemodynamic parameters, duration of anesthesia and the side effects. Ropivacaine being lipophillic, is thought to be less toxic than bupivacaine for the nervous and cardio vascular system.3 These properties are of particular importance during caesarean section and therefore the aim of this study was to establish whether plain isobaric ropivacaine is superior to bupivacaine for spinal anaesthesia during elective caesarean section when equipotent concentrations are used. In our study intrathecal 0.75% isobaric ropivacaine was compared with 0.5% hyperbaric bupivacaine in adult patients undergoing elective and emergency cesarean surgery.
METHODS Our study was prospective, single-blind study, performed on pregnant women scheduled for elective caesarean section after obtaining valid written informed consent. 100 ASA I or II patients were randomized to receive either 2 ml of isobaric 0.75% ropivacaine (n= 50, group R) or 2 ml of hyperbaric plain 0.5% bupivacaine (n=50, group B). patients included in the study were term parturient measuring height of 155 to 165 cm with singleton pregnancy undergoing elective Caesarean section. Exclusion during the study was planned if general anaesthesia was needed. The patients were blinded to group assignment. All patients were administered 10 – 15 ml/kg of crystalloid solutions 30 minutes before the blockade. Spinal anaesthesia was performed in a left lateral position at the L3-L4 or L2-L3level. Quinke’s 26G spinal needle was used. After intrathecal injection, patients were positioned in supine immediately with the table tilted 15° to the left side. Supplemental oxygen was administered via face mask before the delivery in all patients and also later if the oxygen saturation was lower than 92%. Once the patient was returned to the supine position, sensation was assessed by the loss of sharp sensation by using a pinprick test, was recorded bilaterally at the mid clavicular line. The scale usedis as follows: 0 – significant pain, 1 – feeling of touch or minor discomfort and 2 – complete lack of sensation in the operative area. Motor blockade was assessed with the use of the Bromage scale in 5-minute intervals during the procedure, starting from the moment when local anaesthetic was injected intrathecal, until the complete regression of the mo- tor blockade was noted (0 level in the Bromage scale). Surgical procedure was started 10 minutes following the spinal injection to allow for recording of observations. Sensory blockade was assessed by recording every minute during the first 10 minutes after placement of local anaesthetics, and every 5 min there after till the procedure was completed and continued until the complete regression of the blockade was noted. Spread of the sensory blockade up to the T8 level was considered satisfactory for caesarean section. Time required to achieve analgesia was taken from the placement of local anaesthetic agent till the moment when surgical analgesia was obtained. Regression of the blockade was noted, when the patient regained a normal feeling of pain (scale 0)Time between the injection of the local anaesthetic and the full regression of the sensory blockade was regarded as the time of sensory blockade. Time between the injection of the local anaesthetic and the full regression of the motor blockade was regarded as the time of motor blockade. Assessment of motor block were performed at every 5 min initially and later it was done at 10, 20, and 30 min, thereafter at 15-min intervals until the motor block had completely recovered. Parameters of the cardiovascular system (heart rate, systolic blood pressure, diastolic blood pressure, mean blood pressure) and saturation were monitored before and after anaesthesia and was continued in the early postoperative period. Measurements were made 10 min before the blockade and at the interval of 5min. Haemodynamic observation for the purpose of the study was terminated when the full regression of the blockade was noted. All patients received 1 mg of midazolam iv after delivery. Hypotension (systolic arterial pressure <90 mm Hg decreased more than 20% from the initial value) was treated with 6 mg increments of mephentermine IV. Bradycardia (heart rate <50 bpm or decreased more than 20% from the initial value) was treated with IV atropine 0.5 mg. In cases when the patient complains of pain or discomfort was given intravenous injection of ketamine 0.25 mg/kg. The use of all interventional drugs as well as the incidents of nausea and/or vomiting were noted. Each newborn was assessed by the paediatrician with the use of the Apgar score – one minute, five minutes, and ten minutes after the delivery. Data are expressed as mean and standard deviation. Student t test (two tailed, independent) has been used to find the significance of study parameters on continuous scale between two groups Inter group analysis) on metric parameters, Mann Whitney U test has been used to find the significance between two groups for parameters on non-interval scale Chi-square/ Fisher Exact test has been used to find the significance of study parameters on categorical scale between two or more groups. For all calculations p<0.05 was considered statistically significant.
RESULTS Table 1: Demographic data-1-1
Table 2: Characteristics of SAB-1-1
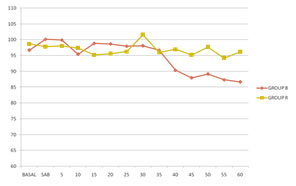
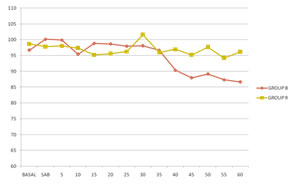
Patients in both groups were comparable with respect to age, height, weight, and ASA status in demographic data (table 1). After recruitment, randomization, and lumbar puncture, there were no exclusions during the study and no conversion to general anaesthesia. Mean time of the procedure was 45.5 ± 25.0 min. in group R and 50.7 ± 18.4 min. in group B. Figure1: intraoperative bloodpressure Figure 2: intraoperative heart rate
In our study, onset of sensory block at T8 was slightly prolonged with ropivacaine compared to bupivacaine (table 2). Similarly we also noted the onset of complete motor block was delayed with plain ropivacaine compared to bupivacaine. Although both ropivacaine and bupivacaine produced favourable surgical conditions. In our study highest cephalad spread of sensory block was observed till T2 to T4 (table 3), although in these patients motor weakness, respiratory distress or cardiovascular compromise were not noticed. However, motor block regressed faster with ropivacaine compared to bupivacaine in our study. Time of request of analgesia is comparable in both groups. Regression to L1 was shorter in case of ropivacaine group in comparison with bupivacaine. The scores of qualities of anaesthesia were similar in both groups. Good muscle relaxation was observed in all patients in group B and group R. The scores of quality of anaesthesia assessed by surgeons was similar in both the groups. Cardiovascular changes were unremarkable throughout, and similar in the two groups (figs 1 and 2), as were the volumes of fluid and doses of ephedrine administered. No significant difference in the incidence of bradycardia was observed in two groups and they responded easily to injection atropine.
DISCUSSION Results of our study suggest that ropivacaine and bupivacaine are comparable when used to provide intrathecal anaesthesia for caesarean section. We compared 2 ml of 0.5% hyperbaric bupivacaine (10 mg) with 2 ml of 0.75% isobaric ropivacaine (15 mg). We observed that ropivacaine significantly produced slower onset (172.8 ± 82.7sec) than bupivacaine (151 ± 88.30 sec); however, the level of sensory block achieved was similar and the duration of sensory block was significantly lesser with ropivacaine. The findings were similar to the study carried out in elective surgeries under spinal anaesthesia by Whiteside et al.3 Ropivacaine 15 mg in glucose 50 mg ml(-1) provides reliable spinal anaesthesia of shorter duration and with less hypotension than bupivacaine. The recovery profile for ropivacaine may be of interest given that more surgery is being performed in the day-case setting. Our study shows ropivacaine group, onset of motor block (498 ± 289.5) and duration of motor block(94.24 ± 17.58 min) indicates lesser potency on motor nerves and the degree of sensory-motor separation is more as compared with bupivacaine (249 ± 181.3)( 210.62 ± 44.98 min) respectively, which has been supported by similar observations of other studies.4 These observations concur with previous studies of carried out by Whiteside et al,3 who observed mean onset time of motor blockade of 15 min and 10 min and total duration of around 90 min and 180 min with similar dose of hyperbaric ropivacaine and bupivacaine respectively. Probably the most comparable study that could be found in the literature was published by Chung et al5. The authors compared intrathecal administration of plain 12 mg of 0.5% hyperbaric bupivacaine solution with plain 18 mg 0.5% hyperbaric ropivacaine solution in patients scheduled for elective caesarean section. Duration of sensory blockade was significantly shorter after ropivacaineMany researchers have tried local anesthetics other than bupivacaine for central blockade during caesarean section, and wide range of dosage and different concentration, baricity and volumes of the local anaesthetic agents have been studied. Gautier et al6. compared spinal ropivacaine and bupivacaine for caesarean section, found that bupivacaine provided longer duration and more profound blockade. Studies have been conducted to compare the effectiveness of ropivacaine using different concentrations. We also noted ropivacaine group has equally good sensory blocks, favorable profile of sensory/motor blockade and early recovery from motor block compared to bupivacaine. These features of ropivacaine are beneficial for ambulatory surgery. We found no evidence of any late sequelae such as backache or other neurological symptoms in our study. Hence, ropivacaine can be safely recommended in ambulatory surgeries. Earlier studies with isobaric ropivacaine reported to have variable or inadequate block patterns during surgery and confirmed that the addition of glucose to the solution of ropivacaine has better effects for SA. It reduces the proportion of a limited block or more extensive block which has been previously reported from studies. Wong et al7, concluded that either 18.75 mg (2.5 ml) or 22.5 mg (3 ml) 0.75% glucose-free ropivacaine could provide spinal anesthesia of the same efficacy and safety for Caesarean section in Chinese women. Ogun et al8. suggested that intrathecal isobaric ropivacaine 0.5% 15 mg plus morphine 150 μg provided sufficient anesthesia for Caesarean delivery and the ropivacaine–morphine combination resulted in a shorter motor block, similar sensory and postoperative analgesia with respect to the same combination of bupivacaine–morphine. In our study, although we used plain ropivacaine that was glucose free and we did not make any analgesic combinations, we achieved sufficient spinal anesthesia. In the study conducted by Wille9, concludes that administration of isobaric ropivacaine in spinal anaesthesia is supported with evidence for the safe use of hyperbaric ropivacaine for cesarean section and day care surgeries.
CONCLUSION 15mg 0.75% isobaric ropivacaine provides safe and equally effective spinal anaesthesia with reduced duration of motor block, compared to 10 mg 0.5 % hyperbaric bupivacaine for cesarean section.
REFERENCES
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.