 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 11 Issue 1 -July 2019
Comparison of ultrasound guided peripheral nerve block and peripheral nerve block for pain relief, closed reduction and short bedside procedures in acute trauma patients
G R Rajashree1, R Satheesh Kumar2*, Samuel Prabakaran3
1Professor, 2PG, Department of Anaesthesiology, Institute of Anesthesiology and Critical Care, Rajiv Gandhi Government General Hospital, Chennai, Tamil Nadu, INDIA. Email: dr.rajashree@hotmail.com
Abstract Background: In our trauma care centre at Rajiv Gandhi Government General Hospital, Chennai, we receive around 2000 cases per month, 100 cases per day, ranging from Polytrauma, both bone fracture upper limb, lower limb and digits, muscle injury, tendon injury among other injuries. Bedside procedures like closed reductions, manipulations and suturing are common in our trauma care centre. Peripheral nerve blocks without any delay can be a blessing in reducing the pain during these bedside procedures. Materials and Methods: 50 patients with the various trauma mentioned above were divided into two groups, group U and group B. Patients in group U received ultrasound guided peripheral nerve blocks depending on site of injury, within 30 minutes of arrival in trauma ward with equal volume of 0.25% bupivacaine and 1% lignocaine, not exceeding the dose calculated based on weight of patient . The other group received blind peripheral nerve blocks depending on site of injury, within 30 minutes of arrival in trauma ward. The patients chosen were of Age 20 years to 70 years, Glasgow coma scale: 15/15, Body Mass Index <40, not allergic to local anaesthetics and Who have given valid informed consent. Conclusion: We conclude that adequate analgesia was achieved in both groups for bed side procedures to be done without any sort of pain and duration of analgesia and recovery was similar. Failure rate was lesser in case of ultrasound group. Keywords: Trauma, USG Machine, Nerve block needles, Local anaesthetics
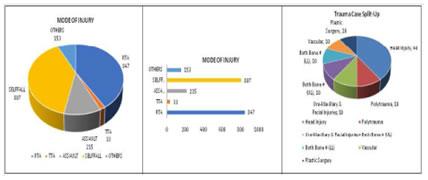
INTRODUCTION In our trauma care centre at Rajiv Gandhi Government General Hospital, Chennai, we receive around 2000 cases per month, 100 cases per day, ranging from Polytrauma , both bone fracture upper limb, lower limb and digits, muscle injury, tendon injuryamong other injuries. Extremities are the most commonly injured parts with the advent of head and torso protection devices in modern vehicles. Analgesia is often unjustifiably delayed even in patients without serious injuries. Bedside procedures like closed reductions, manipulations and suturing are common in any trauma care centre. The following picture depicts the scenario of trauma cases in our trauma care setup. Management of pain in acute trauma patients is challenging. The pain associated with injury is not given adequate thought. Pharmacological pain management especially systemic opioids have several disadvantages like causing hemodynamic instability or respiratory depression and airway compromise. Even though multimodal pharmacological management has lesser chance of serious side effects than only opioids, peripheral nerve blocks have been proven to be superior. Peripheral nerve blocks also have the added advantage of improved ability to perform neurological assessment, improved transport and cost savings. The various peripheral nerve blocks that are performed are supraclavicular, axillary, forearm, wrist, digits, femoral, sciatic, adductor canal, popliteal, ankle and toe blocks depending on the site of injury.Landmark based blind peripheral nerve blocks have historically long been practiced in acute trauma setup. The advent of ultrasound in peripheral nerve blocks has significantly improvedsuccess rate and drastically reduced complication rate.Timely analgesia added with the safety of peripheral nerve blocks will provide adequate analgesia, help perform afore mentioned bedside procedures with ease and improve patient recovery. Evidence supporting peripheral nerve blocks in acute trauma setup is very weak at present and requires properly powered randomized controlled studies.
MATERIALS AND METHODS The study was conducted in Rajiv Gandhi Government General Hospital, Madras Medical College, Chennai after a pilot study of 10 cases each. After obtaining approval from the institutional ethics committee written informed consent was obtained from patients and relatives. Patients included were 20-60 years, GCS 15/15, BMI<40, not allergic to local anaesthetics and who have given informed consent with similar injuries. Patients excluded were unconscious patients, severe head injury, bleeding disorders and coagulation abnormalities, hemodynamically unstable, seizure disorder, patients with severe cardiovascular, endocrine, respiratory, renal and hepatic disorders, pregnant and lactating mothers. Monitors included were non invasive blood pressure, ECG and pulse oximeter. After randomization patients with similar injuries were allocated into two groups (Group U- Ultrasound guided peripheral nerve blocks, Group B- Blind peripheral nerve blocks). Each group received their blocks within 30 minutes of arrival. Equal volumes of 0.25% bupivacaine and 1% lignocaine without adrenaline was used as per the body weight. Depending on the site of injury , supraclavicular(30 ml), axillary(25ml), forearm(25ml),wrist(20ml), digital(10ml),femoral(10ml), sciatic(30 ml), adductor canal(25ml) or ankle block(30ml) was given using 5/10 cm atraumatic needle.They were monitored with HR, BP, SpO2 and visual analogue score assessment half hourly for 3 hours and then hourly for next 3 hours. The collected data was analysed with IBM SPSS statistics software which includes tests like Shapiro wilk’s test, unpaired sample t test, ANOVA and Chi-square test.
RESULTS Out of 100 patients assessed for eligibility, they were randomized according to the study protocol. In all the statistics, the probability value of 0.05 is considered as significant level.
Table 1:
The age range distribution between Group U and Group B shows there is statistical significance (P = 0.698). This was due to the study being conducted in a trauma centre where blocks were given as and when the patients got admitted randomly without categorically dividing patients.
The gender distribution between Group U and Group B shows there is statistical significance (P = 0.54). This was due to the study being conducted in a trauma centre where blocks were given as and when the patients got admitted randomly without categorically dividing patients. Table 3: Variability of Heart rate in both groups
Table 3 shows that the comparison between Group U and Group B in heart rate shows no statistical significance in all the time period except in the ½ hour mark. Table 4: Changes in Systolic blood pressure
The comparison between Group U and Group B in systolic BP shows no statistical significance in the first 3 hours and was statistically significant from the 4th hour. Table 5: Changes in Diastolic blood pressure
The comparison between Group U and Group B in diastolic blood pressure shows no statistical significance in all the time period except in the 5 hour mark. Table 6: Changes in spO2
The comparison between Group U and Group B in spO2 shows statistical significance in all the time period. Table 7: Changes in VAS score
The comparison between Group U and Group B in VAS shows statistical significance in the first hour and from 4th – 6th hour.
DISCUSSION Randomly selected patients were given peripheral nerve blocks using both blind and ultrasound guided techniques. Gender distribution showed male patients were more than the females which was reflective of the general trend in our trauma care setup. The age of the patients that underwent blind nerve blocks was found to be more than ultrasound group which was reflective of the random selection of the patients. The differences in heart rate, systolic and diastolic BP between both the groups were not statistically significant for most of the time period. The comparison in VAS score between the two groups showed 2 sets of statistical significance. The statistical significance in the first hour is indicative of the increased failure rate in the blind group. The statistical significance in the 4th – 6th hour is indicative of the slightly lesser duration of analgesia in blind group.
CONCLUSION Peripheral nerve blocks have been proven to successfully alleviate pain in the acute trauma patient and facilitate closed reduction, suturing of muscles and superficial layers after adequate analgesia. The study shows that ultrasound guided nerve blocks are more accurate and result in increased duration of analgesia when compared to blind technique. REFERENCES
. |
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.