 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 11 Issue 1 -July 2019
Comparison of granisetron and ketamine in prevention of post operative shivering in patients undergoing regional anaesthesia
Darshan Bhatt1, Divya Mahajan2*, Ravi Goel3, Nishi Kulshreshtha4
1Consultant Anaesthetist, Zydus Hospital, Anand, Gujarat, INDIA. Email: darshanbhatt1990@gmail.com, rg2565@gmail.com ,drnishi_kul@yahoo.com
Abstract Background And Objectives: Shivering during neuraxial anaesthesia has detrimental effects. It is distressing to the patient recovering from the effects of anaesthesia, both psychologically and physiologically. This study aims to compare efficacy of ketamine and granisetron in prevention of post anaesthetic shiveringin patients undergoing regional anaesthesia. Method: After approval by the Hospital Ethics Committee, the study was conducted on 80 adult ASA Grade I or II patients (40 in each group) of either sex in the age group 18 to 60 years admitted on our hospital, who underwent elective surgeries under spinal anaesthesia. Patients in group K received ketamine 0.5 mg/kg and patients in group G received 40 μg/kg granisetron just after intrathecal injection of hyperbaric bupivacaine. Sample size was calculated using MedCalc Software version 11.5.0.0. (MedCalc Software bvba, Acacialaan 22, 8400 Ostend, Belgium) Result: Shivering scores were higher in group G as compared to group K during intraoperative period. (P value < 0.05). In postoperative period, differences were observed for the period of initial 15 minutes. Thereafter both groups were comparable. In postoperative period no patient had grade 3 or 4 shivering in both the groups. Intraoperatively, at all time intervals, sedation scores were significantly higher in group K as compared to group G. Conclusion: In early postoperative period ketamine more effectively reduces shivering as compared to granisetron, although with higher sedation scores. However both are equally efficacious in reducing postoperative shivering in late postoperative period without any side effects. Key Words: Regional Anaesthesia, Ketamine, Granisetron, Post operative Shivering
INTRODUCTION Shivering is encountered both after regional and general anaesthesia. The combination of anaesthetic induced thermoregulatory impairment and exposure to a cool environment makes most unwarmed surgical patients hypothermic1. Regional anaesthesia impairs thermoregulatory control and the incidence of shivering during regional anaesthesia is up to 57 percent2. It causes vasodilatation which facilitates core to peripheral redistribution of heat leading to shivering3.Shivering is uncomfortable and is perceived by many as equivalent to the postoperative surgical pain. It can hamper the normal smooth recovery and can be detrimental in certain group of patients like patients with raised intraocular pressure, raised intracranial tension and with limited cardiorespiratory reserves4. Recently, 5-hydroxytryptamine 3 (5-HT3) receptor antagonists have been reported to prevent post anesthetic shivering. Serotonin (5-Hydroxytryptamine), has a role in neurotransmission and studies suggest that the serotonergic system has a role in control of postanaesthetic shivering5. Granisetron, a 5-HT3 receptor antagonist, has been shown to be effective in preventing shivering under regional anaesthesia. Ketamine is a competitive NMDA receptor antagonist and has a role in thermoregulation at various levels. It decreases core to peripheral redistribution of heat. NMDA receptor modulates noradrenergic and serotoninergic neurons in locus coeruleus. It has been used as antishivering agent. But it also increases arterial pressure, heart rate and cardiac output because of direct central sympathetic stimulation. Various studies have demonstrated efficacy of ketamine and granisetron in prevention of postoperative shivering in patients undergoing regional anaesthesia. Aim of this study is to compare the efficacy of ketamine and granisetron in prevention of postoperative shivering in patients undergoing surgeries under regional anaesthesia.
METHODS This prospective Interventional study, which was approved by Ethics Committee, included patients between 18 and 60 years of age , American Society of Anaesthesiologist (ASA) I and II patients scheduled for lower abdominal surgeries under spinal anaesthesia. Patients allergic to drugs used in regional anaesthesia, ASA III and IV, obese patients and those with preoperative temperature > 38 °C or <36.5 °C were excluded from the study. Primary Hypothesis: Our primary hypothesis was that both ketamine and granisetron are equally efficacious in preventing post operative shivering .The study was conducted from 2014 to 2015 .Sample size was calculated using MedCalc Software version 11.5.0.0. Forty patients in each group were considered adequate with 2-sided type 1 error of 0.05 and 90% power to detect a significant difference between the groups. The study participants were randomly divided into two groups of forty patients each (n = 40) using computer generated random number list , Ketamine group(Group K) and Granisetron group(Group G).A thorough pre anaesthetic check up was done one day prior to the surgery. The anaesthetic procedure was explained to the patient in detail and written informed consent was taken. All routine biochemical, hematological and radiological investigations were done as per our hospital protocol. Routine preoperative preparation consisted of fasting for 6-8 hours prior to surgery. All the patients were given tablet alprazolam 0.5 mg night before the surgery.In the preop room, all the vitals including axillary temperature were observed and recorded into the proforma. Axillary temperature was used due to unavailabilty of tympanic probe.In the operation theatre, all the baseline parameters such as heart rate (HR), electrocardiography (ECG), non-invasive blood pressure (NIBP), pulse oximetry (SpO2), and axillary temperature were recorded and an intravenous (IV) access was secured with a venous cannula preferably in nondominant hand. Intravenous fluids in form of NS /RL warmed to 37 °C were infused as maintenance fluid. Anaesthetic management included subarachnoid block instituted at either L3/4 or L4/5 interspaces using standard midline approach with hyperbaric bupivacaine 5mg/ml, 10-15mg injected using 25G quincke spinal needle. Vitals were recorded immediately after the subarachnoid block. Group K and Group G patients received a diluted solution of 4ml of normal saline containing 0.5mg/kg ketamine and 40 μg/kg granisetron, respectively, given intravenously just after intrathecal injection. During perioperative period height of sensory block was assessed with pinprick test after 5min. Supplemental oxygen 5 litres/min was delivered via facemask during the operation. Axillary temperature was measured after intrathecal injection and thereafter every 15 minutes. All the patients were covered and operation room temperature was maintained at 22-25°C. All the vital parameters were duly observed and recorded into the proforma.In the recovery room, all the patients were covered with warm blankets and their axillary temperature was recorded on arrival. They were given oxygen @ 5 L/min in a slightly propped-up position. Recovery room temperature was maintained between 22-25°C.All cases were screened for shivering if any, and graded with a 5 point scale validated where – 0 = No shivering, 1 = Piloerection or peripheral vasoconstriction but no visible shivering, 2 = Muscular activity in only one muscle group, 3 = Muscular activity in more than one muscle group, 4 = Whole body shivering. Any episode of shivering, fever, pain, hallucination, dry mouth, postoperative nausea and vomiting (PONV) and other complications was recorded.
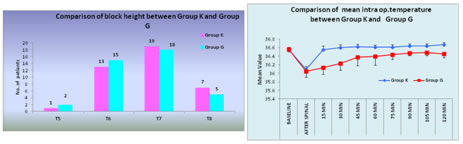
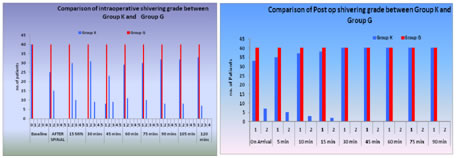
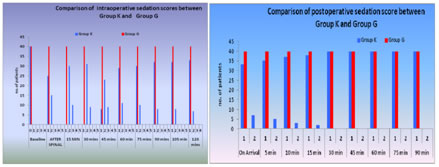
RESULTS Figure 1 Figure 2 Figure 3 Figure 4 Figure 5 Figure 6 Figure 1: Comparison of block height between group k and group G; Figure 2: Comparison of mean intraoperative temperature between Group K and Group G; Figure 3: Comparison of intraoperative shivering grade between both groups; Figure 4: Post operative shivering scores in both groups; Figure 5: Intraoperative sedation scores in both groups; Figure 6: Comparison of postoperative sedation score between Group K and Group G
Eighty patients completed the study protocol. There was no statistically significant difference concerning age, gender, height, weight, ASA status and duration of surgery between the two groups OUTCOME VARIABLES BLOCK HEIGHT Figure 1 shows comparison of block height between group K and G Comparing two groups, there was no statistical difference between two groups (P value = 0.841) TEMPERATURE Trends in mean temperature at various time intervals in both groups are summarized below. A. Intra operative Comparing two groups, baseline temperature was comparable in both groups. (P value= 0.452). 15 min after administration of spinal anaesthesia mean temperature in group K was higher as compared to group G.( p value = <0.001). The trend continued with mean temperatures in group K remaining significantly higher (p value = <0.001) in comparison to group G at all time intervals during intraoperative period as shown in figure 2. B. Post operative Comparing two groups, mean temperatures in group K were significantly higher than those in group G during all time intervals in postoperative period. (P value = <0.005) SHIVERING SCORE INTRA OPERATIVE PERIOD Comparing both groups, as depicted in figure 3, baseline shivering scores were same in both groups. Shivering scores were higher in group G as compare to group K at all time intervals during intraoperative period. (P value<0.05)
POSTOPERATIVE PERIOD On comparing two groups, statistically significant difference was observed between two groups in early post operative period till 15 min,( p value <0.05). After that no significant difference was observed as shown in figure 4. Intraoperative period Intra operative sedation scores(figure 5) were significantly higher in group K as compared to group G at all time intervals during intraoperative period. (P value = < 0.05) Post operative period Comparing two groups, as shown in figure 6, sedation scores were significantly higher in group K (p value< 0.05) till 10 min to arrival to recovery. After that no significant difference was observed. MEAN HEART RATE AND MEAN MAP Intra operative period Baseline mean heart rates and mean MAP were comparable in both groups. Intra operative heart rates and mean MAP were comparable in both groups during all the time periods. (P value > 0.05) Post operative period Mean heart rates and mean MAP were comparable in both the groups on arrival to recovery with p value of 0.128 and 0.417 respectively and at all time intervals during post operative period(P value > 0.05). INCIDENCES OF SIDE EFFECT In group K significant hypotension requiring ephedrine bolus of 5 mg occurred in 2 out of 40 patients. In group G 4 patients had significant hypotension requiring ephedrine bolus of 5 mg. Comparing two groups, no significant difference was seen. (P value = 0.675)In group K 1 patient had nausea which resolved spontaneously without requiring any treatment. Vomiting was not seen. No patient in group G had nausea or vomiting. Comparing two groups, the difference was not significant. (P value = 1.000).
DISCUSSION From our study, we conclude that in early postoperative period, ketamine ( 0.5mg/kg ) more effectively reduces shivering as compared to granisetron (40 μg/kg ), whereas in late postoperative period both were found to be equally efficacious. During the post operative period, shivering is a frequent and undesirable complication of anaesthesia. A number of factors including age, level of sensory block, temperature of used local anaesthetic, temperature of the operating room and infusion solution are risk factors for hypothermia in regional anaesthesia. For these reasons, patients over the age of 60 years were excluded from the study, the temperature of the operating room was maintained at 24°C and infusions of cold crystalloid solutions were avoided. Shivering increase metabolic activity and oxygen consumption. It may also cause arterial hypoxia and lactic acidosis. Furthermore, it may interfere with the monitoring of an electrocardiogram. All of these make the prevention of shivering important especially in elderly patients with a low cardiopulmonary reserve.13Pharmacological therapies such as pethidine, tramadol, physostigmine and clonidine have been used to prevent shivering. However as the incidence of hypotension is high during regional anaesthesia, hypotensive agents including clonidine and urapidil may not be suitable in preventing shivering. Also tramadol and pethidine may not be suitable during and after regional anaesthesia because of their potential to cause nausea and vomiting and respiratory depression. The agents used for the treatment of shivering during regional anaesthesia should not cause nausea and vomiting or hemodynamic instability. Ketamine, an NMDA receptor antagonist, also inhibits and prevents perioperative shivering. It is likely that NMDA receptor antagonist modulates thermoregulation at a number of levels. In addition to being competitive NMDA receptor antagonist, ketamine has several other pharmacological properties; these include - being a k-opioid agonist, biogenic amine uptake in the descending inhibitory monoaminogenic pain pathway, having a local anaesthetic like action and interaction with muscarinic receptors. Therefore, it probably controls shivering by non- shivering thermogenesis either by action on the hypothalamus, or by b -adrenergic effects ofnorepinephrine.9Ketamine has been shown to prevent shivering without hemodynamic alterations in patients undergoing regional anaesthesia. It probably controls shivering by non-shivering thermogenesis either influencing the hypothalamus or by the beta adrenergic effect of norepinephrine. However, patients may develop hallucinations and post operative nausea and vomiting. Granisetron, 5-HT3 receptor antagonist, is effective in the prevention of post operative shivering in regional anaesthesia as observed by Asif Iqbal. 5-hydroxytryptamine may influence both heat production and heat loss pathways.6SHIVERING GRADES O.Sagir et al7 noted higher shivering scores in granisetron group as compared to ketamine group, 15 min after spinal anaesthesia with p value of <0.02. Our study also had same finding at similar time interval. In a study by B.Shakya et al 8 15 min after spinal anaesthesia, 1 patient in ketamine group had shivering. In our study also we had 1 patient with grade 1 shivering in ketamine group. Findings in our study were also comparable with the studies carried out by A .Honarmand et al.10 In the early post operative period , shivering scores in ketamine group were lower, while in late post operative period , no significant difference was seen. In a study by D. Dal et al11 no patients in ketamine group had shivering in postoperative period. Asif Iqbal et al6 and Gecaj-Gashi A et al 12 also had similar results SEDATION SCORE During spinal and local anaesthesia, intravenous sedation and hypnotic drugs are often administered to increase patient comfort, to maintain cardio respiratory stability, to improve surgical condition and to prevent recall of unpleasant events during surgery.9Intra operative sedation scores were significantly higher in group K as compared to group G. In their study O.Sagir et al 7 also noted significantly higher sedation scores in ketamine group (median 2) as compared to granisetron groups (median 1), 15 min after spinal anaesthesiaIn studies by A.Honarmand et al10 and B.Shakya et al 8 higher intraoperative sedation was seen in patients in ketamine group. In this connection, the patients of Group K have more perioperative comfort than group G.Srikanta Gangopadhyay et al 9 also noted higher postoperative sedation score in ketamine group as compared to tramadol and pethidine groups, though they used different sedation scale. In our study also we noted higher sedation grades in ketamine group. TEMPERATURE SIDE EFFECTS In group K significant hypotension requiring ephedrine bolus of 5 mg occurred in 2 out of 40 patients. In group G 4 patients had significant hypotension requiring ephedrine bolus of 5 mg. Comparing two groups, no significant difference was seen. (P value = 0.675)In a study by O.Sagir et al 7, in granisetron group 8 patients had hypotension as compared to 3 in ketamine group, difference between two groups being statistically insignificant. In group K 1 patient had nausea which resolved spontaneously without requiring any treatment. Vomiting was not seen any of the patient. Similar findings were seen in studies of D. Dal et al 11, Srikanta Gangopadhyay et al 9 and Gecaj-Gashi A et al 12. No patient in group G had nausea or vomiting which was similar to the findings of Asif Iqbal et al.6
CONCLUSION From our study, we conclude that in early postoperative period, ketamine more effectively reduces shivering as compared to granisetron, although with higher sedation scores. However both are equally efficacious in reducing postoperative shivering in late postoperative period without any side effects.
REFERENCES
. |
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.