.
A comparative study between fentanyl and nalbuphine as an adjuvant to hyperbaric bupivacaine in spinal anaesthesia for elective lower abdominal and lower limb surgeries
A Ashwini1*, M S Priyanka2, S Nethravathi3, Nabeela Basri4
1Associate Professor, 2,3,4Junior Resident, Department of Anaesthesiology, Kempegowda Institute of Medical Sciences and Research Center, Krishna Rajendra Road, Parvathipuram, Vishweshwarapura, Basavanagudi, Bengaluru, Karnataka.
Email:dr.ashwinivijay.a@gmail.com
Abstract Background: Opioids have been favored as adjuncts to local anesthetics during spinal anesthesia, one among them commonly used is fentanyl. However Nalbuphine, a mixed agonist–antagonist opioid and a potent analgesic in less explored for analgesia. Hence this prospective double blind study was done to compare and evaluate the characteristics of spinal block using fentanyl and nalbuphine as adjuvants along with 0.5% bupivacaine in patients undergoing elective lower limb and lower abdominal surgeries. Methods: In our randomized comparative study, 100 patients aged between 18-60 years of ASA 1 and 2 undergoing elective lower abdominal and lower limb surgeries were included, after ethical clearance. Two groups of 50 each were randomly allocated by computer generated random number table, Group F received 2.5ml of intrathecal 0.5% hyperbaric bupivacaine with 25mcg of fentanyl and Group N received 2.5ml of 0.5% hyperbaric bupivacaine with 0.5mg nalbuphine. Onset of sensory and motor blockade, duration of motor blockade and analgesia were noted in both the groups. Sedation scores and side effects were evaluated. Statistical analysis was done by student` s t test and Chi- square test. Results: The mean time of onset of sensory block and motor block was significantly faster in Nalbuphine group as compared to fentanyl group(p <0.001). The time of two segment regression of sensory blockade, total duration of motor blockade and duration of analgesia was significantly prolonged in Nalbuphine group. Sedation scores were higher in nalbuphine group. No significant differences were noted in hemodynamic variables. Conclusion: Intrathecal Nalbuphine hastens the onset of sensory and motor blockade and significantly prolongs the two segment regression, total duration of sensory and motor blockade with optimum sedation and with no side effects in comparison with intrathecal fentanyl.
Key Word: Spinal anesthesia; Fentanyl; Nalbuphine; Adjuvant; Efficacy
INTRODUCTION
Spinal anesthesia is the best regional anesthetic technique for lower abdominal and lower limb surgeries, as it is simple to perform, faster in onset and provides complete muscle relaxation1. Its major disadvantage is shorter duration of action and decreased postoperative pain relief2. To overcome these short coming various adjuvants are added to local anesthetics. They improved the quality and duration of spinal blockade, prolonged post operative analgesia and also reduced the requirement of dose and amount of local anesthetic. Opioids are one among such adjuvants having synergistic action with local anesthetics and intensify the sensory blockade3 without increasing sympathetic blockade3. The rationale of adding opioids to local anesthetics is that these two types of drugs act at two different sites to eliminate pain. Local anesthetics act on neuronal axons and the opioids act on their receptor sites to produce analgesia4. Fentanyl is a lipophilic opioid and mu receptor agonist, which on intrathecal injection has rapid onset, improves quality of anesthesia, post-operative analgesia, hemodynamic stability without producing significant side effects. It is a commonly used opioid adjuvant with intrathecal bupivacaine1-3. Nalbuphine, a mixed agonist-antagonist opioid, antagonizing mu receptor activity and enhancing kappa receptor effects. It was synthesized in intent to produce analgesia without side effects of mu agonist. Very few studies have been done using intrathecal Nalbuphine as an additive to 0.5% Bupivacaine. Hence this study to evaluate and compare the characteristics of spinal block and the effects of intrathecal bupivacaine with fentanyl and bupivacaine with nalbuphine in adult patients undergoing elective lower abdominal and lower limb surgeries.
MATERIALS AND METHODS
After approval of the Ethical Committee clearance and after taking patients written informed consent. Hundred adult patients coming to KIMS Hospital for elective lower abdominal and lower limb surgeries were selected.
Inclusion Criteria: Age group between 18-60yrs of either sex, ASA 1 and 2, weight:50-80kg, height: >150cm.
Exclusion Criteria: patient refusal, pregnancy and lactation, patient with obesity, allergic to local anesthetics, local infection, severe hypovolemia, coagulation abnormalities, neurological disorders.
The patients were divided randomly using computer generated number and concealed using sequentially numbered, sealed opaque envelope technique into two equal groups (each 50 patients): Group F and Group N. All patients were clinically assessed and routine and relevant preoperative investigations were done. All patients were pre-medicated with Tablet alprazolam 0.5 mg and Tablet Rantac 150mg overnight and morning on the day of surgery. Patients were kept nil orally for a period of 8 hours. The monitors (electrocardiography, non-invasive blood pressure and pulse oximetry) were connected to the patient on arrival to the operating room and basal parameters were recorded. A suitable peripheral vein was cannulated and I.V. Ringer solution 10 ml/kg/15 min (preload) was given to all patients before the procedure. All patients were put in the either right or left lateral position. Under aseptic precaution, dural puncture was performed at L3–L4 or L4–L5 interspace with a 26 gauge Quincke spinal needle. The patients were divided equally into two groups according to the additive (fentanyl or nalbuphine), and all patients divided Group N (n-50)/50 patients received intrathecal injection of 2.5ml of 0.5% hyperbaric bupivacaine with 0.5mg nalbuphine(0.5ml) total 3ml Group F(n-50)/ 50 patients received intrathecal injection of 2.5ml of 0.5% hyperbaric bupivacaine with 25mcg fentanyl (0.5ml) total 3ml Subarachnoid block were performed by anesthesiologists who did not participate in recording patients’ data. Both patients and observers were blinded to the drugs given. Then, the patients were placed in the supine position with elevation of the head by a pillow and oxygen mask 5 l/min was applied. Continuous monitoring of the conscious level and oxygen saturation were done. The level of sensory block (assessed by pin prick) and motor block (assessed by Bromage scale; 0 = none, 1 = just able to move the knee but not the hip, 2 = able to move the foot only, 3 = unable to move the knee or foot) were continuously recorded until skin incision. Surgery began when the adequate block was achieved. Heart rate and blood pressure were measured noninvasively every minute for the first 5 minutes, then every 5 minutes for the next one hour and then every 15 minutes till the end of surgery. Thereafter monitored for every 30 minutes. Atropine (0.01 mg/kg) was given if H.R. decreased below 60/min. Intermittent doses of ephedrine 6 mg I.V. if the systolic arterial blood pressure decreased by more than 20% below preanesthetic level or less than 100mmHg. Visual analog scale (VAS) was recorded [it ranges from 0 indicating no pain till 10 indicating severe intolerable pain with variable degrees of ascending pain in between]. If VAS > 4, general anesthesia was given and the patient was excluded. Any adverse events such as pruritus, nausea, vomiting were noted and treated accordingly. In the PACU, vital parameters were noted every 30minutes. Recovery from sensory and motor blockade were noted. The duration of analgesia was recorded. The time of rescue analgesia was recorded. NSAIDs were given for analgesia to all patients scoring VAS>5 according to the ward protocol.
Statistical methods: Descriptive and inferential statistical analysis has been carried out in the present study. Results on continuous measurements are presented on Mean±SD (Min-Max) and results on categorical measurements are presented in Number(%). Significance is assessed at 5% level of significance. Student t test (two tailed, independent) has been used to find the significance of study parameters on continuous scale between two groups (Inter group analysis) on metric parameters. Leven1s test for homogeneity of variance has been performed to assess the homogeneity of variance. Chi-square/ Fisher Exact test has been used to find the significance of study parameters on categorical scale between two or more groups, Non-parametric setting for Qualitative data analysis. Fisher Exact test used when cell samples are very small. For all calculations p<0.05 was considered statistically significant
Statistical software: The Statistical software namely SPSS 18.0, and R environmentver.3.2.2 were used for the analysis of the data and Microsoft word and Excel have been used to generate graphs, tables etc.
RESULTS
Table 1: Demographic data and duration of surgery of the two studied groups
characteristics |
Group F |
Group N |
P value |
Age (years) |
38.88 ± 8.17 |
39.10± 11.46 |
0.912 |
Height (cm) |
161.30± 7.42 |
162.30±6.88 |
0.486 |
Weight (kegs) |
64.24± 8.75 |
66.34±9.45 |
0.252 |
Duration of surgery(minutes) |
101.05 ± 29.33 |
96.32 ±21.11 |
0.356 |
Data are expressed as mean standard deviation. There were no statistically significant differences among the two groups regarding age, height, weight and duration of surgery.
Table2: Sensory block, motor block and duration of analgesia of the two studied groups
characteristics |
Group F |
Group N |
p value |
Onset of sensory block (min) |
2.20± 0.57 |
1.38 ± 0.53 |
< 0.001 |
Onset of complete motor block(min) |
5.36 ± 0.63 |
3.72± 0.64 |
< 0.001 |
Two segment regression time of sensory block(min) |
93.54± 5.08 |
110.68 ± 6.51 |
<0.001 |
Duration of motor block(min) |
155.80 ± 7.47 |
170.48 ±7.42 |
<0.001 |
Duration of analgesia(min) |
217.98±21.66 |
261.80 ±9.5 |
<0.001 |
Time taken for the onset of sensory block in the Group F was 2.20±0.57 minutes and in the Group N was 1.38±0.53 minutes. The onset time of sensory block in group N was statistically significant and was earlier in onset in comparison to group F as indicated by the ‘p’ value<0.001. The mean time for onset of motor blockade (modified Bromage 3) was 5.36±0.6 3minutes in Group F and 3.72±0.64 minutes in Group N respectively. Mean duration of onset of motor blockade of Group N was earlier and was statistically significant in comparison with group F with p value <0.001. The mean duration of motor blockade in group F was 155.80±7.47 minutes and group N was 170.48±7.42 minutes. The duration of motor blockade was prolonged in Group N in comparison to Group F. This was statistically significant with a p value<0.001** The mean time for two segment regression in the group F was 93.54±5.08 minutes and in group N was 110.68±6.51 minutes. There was a significant prolongation of time for 2 segment regression in group N in comparison with group F as indicated by the ‘p’ value < 0.001.The mean duration of analgesia in group F was 217.98±21.66 minutes and that in group N was 261.80±19.58 with ‘p’ value <0.001. Group N had significantly long duration of analgesia in comparison to Group F which was statistically significant.
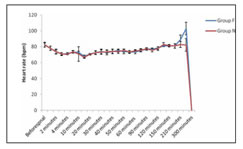
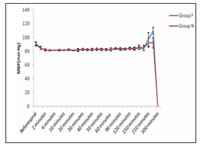
Figure1 Figure 2
Figure1:Comparison Of Heart Rate In Two Groups Of Patients Studied; Figure 2: Comparison of MBP (mm Hg) in two groups of patients studied
The heart rate variability at various intervals were compared. There was statistically significant difference in heart rate between the two groups at various intervals but were not clinically significant.
Changes in mean arterial blood pressure recorded at various time intervals in both groups were compared. There was significant difference in the mean arterial blood pressure readings between the two groups at some intervals of time but were not clinically significant and did not need in any treatment.
DISCUSSION
Intrathecal opioids used as adjuvants act synergistically with local anesthetics and intensify the sensory block without affecting sympathetic blockade. We compared 2.5ml of 0.5% Hyperbaric Bupivacaine with 0.5ml (25mcg)Fentanyl and 2.5ml of 0.5%hyperbaric Bupivacaine with 0.5ml(0.4mg)Nalbuphine in patients undergoing elective lower abdominal and lower limb surgeries. We observed in our study that the onset of sensory block in Nalbuphine group was faster compared to fentanyl group which was also observed by Kokum et al5, in his study, who compared intrathecal Nalbuphine versus Fentanyl as adjuvant to 0.5% hyperbaric Bupivacaine and found some difference in onset of sensory block, but was statistically insignificant. Similarly, he commented on the onset of motor blockade, which was also statistically insignificant. But our study showed that the mean onset of motor blockade was faster in Nalbuphine group and was also statistically significant. Onset of action of local anesthetics has been enhanced using adjuvants, in which a study done by Shehla Shakooh et al6, titled Intrathecal Nalbuphine: An effective adjuvant for post-operative analgesia, which showed that the time of onset of sensory blockade in group receiving 0.8mg nalbuphine with 3ml of 0.5% hyperbaric Bupivacaine was 1.43 ±0.57min,which is in accordance with our study, that showed 1.38 ±0.53minutes for onset of sensory blockade with 0.4mg nalbuphine with 2.5ml of 0.5% hyperbaric Bupivacaine ,proving its potency. Local anesthetics block the transmission of impulses most easily in the smaller, thinly myelinated B fibers carrying sympathetic impulses and non myelinated C fibers carrying pin prick sensation. So, on addition of adjuvants to local anesthetics also enhances its time to reach highest sensory block which was also proved in our study that Nalbuphine and Fentanyl were comparable regarding the time to reach highest sensory block .This was in accordance with the study done by Ravikiran J Thote et al7, who Compared intrathecal Bupivacaine with Fentanyl, (25mcg),Nalbuphine(0.5mg) and plain bupivacaine for lower limb surgeries and proved that the time taken to reach the highest sensory level were comparable and with no much difference. Blockade of the A fibers, the largest motor fibers and medullated proprioceptive fibers, is slower in onset and short duration. So Shagufta Naaz et al8, in his study showed the duration of motor blockade was 177.5 ±50.45min which is in accordance to our study. Motor blockade can be prolonged with addition of adjuvants and its better with Nalbuphine group compared to Fentanyl group. Along with duration, time for two segmental regressions required to be known, for any prolonged upper abdominal surgeries, which was estimated by Padma et al9, in her study, which shows that time for 2 segment regression of sensory level was 115±9.12min with intrathecal nalbuphine with Bupivacaine .This was in accordance with our study, which was about 110.68±6.51min.Similarly using Fentanyl with bupivacaine, Harbhejsingh et al10, showed time for two segment regression was around 93.4 ±22minutes, this was in concordance with our study which was about 93.54 ±0.22 min. Comparatively, Nalbuphine group showed prolonged duration of action and two segment regression compared to fentanyl group. Regional anesthesia also serves the purpose of perioperative and postoperative analgesia which was proven by Ravikiran J Thote et al11., who showed that duration of analgesia was prolonged with Nalbuphine compared to Fentanyl group which was in concordance with our study .In a study done by Manjula R et al12 showed the prolonged duration of action of Nalbuphine which wasabout 260±5.64min with 1mg of Intrathecal Nalbuphine with 3ml of Bupivacaine whereas in our study , duration of action was around 261±19.58min with 0.4mg nalbuphine, which also proved its efficacy. Spinal anesthesia is usually associated with wide variation in hemodynamic variables like heart rate, mean arterial pressure as showed in our study which is statistically significant but they were clinically in normal limits which did not require any clinical intervention. This was similar to the study done by Kanhyahalguptaet al13, titled Efficiency of Nalbuphine as an adjunct to Bupivacaine in lower limb orthopedic surgery.
CONCLUSION
Nalbuphine 0.5mg added to 2.5ml of 0.5% Hyperbaric Bupivacaine produced early clinical onset of sensory and motor blockade when compared to 25 microgram of Fentanyl. The mean time to achieve highest sensory level was comparable in both Nalbuphine and Fentanyl groups. The mean time for two segment regression was significantly prolonged when Nalbuphine was added to Bupivacaine compared to the addition of Fentanyl to bupivacaine. Total duration of motor blockade and duration of analgesia was of significantly longer duration in Nalbuphine group compared to Fentanyl group. The only side effect noted was in Fentanyl group (5 patients) was pruritus which was self-limiting, did not require any treatment also, there was no statistically significant difference in side effects noted between the two groups.
REFERENCES
-
Gomaa H, Mohamed N, Zoheir H, Ali M. A Comparison Between Post-operatives Analgesia After Intrathecal Nalbuphine With Bupivacaine And Intrathecal Fentanyl with Bupivacaine after Cesarean Section. Egyptian Journal Of anesthesia. 2014;30(4):405-410.
-
Thote J. R, Lomate P. Comparison Among Intrathecal Fentanyl And Nalbuphine In Combination with Bupivacaine and plain Bupivacaine for lower limb surgeries. International Journal Of Recent Trends In Science And Technology. March 2015;14(2):361-366.
-
Dhumal P R, Kolhe E P, Synergistic Effect Of Intrathecal Fentanyl And Bupivacaine Combination For Cesarean Section International Journal Of Pharmaceutical And Biomedical Research. 2013:4(1):50-56.
-
Jyothi B, Shaikh S. A Comparison Of Analgesic Effect Of Different Doses Of Intrathecal Nalbuphine Hydrochloride With Bupivacaine And Bupivacaine Alone For lower Lower Abdominal And Orthopedic Surgeries. Indian Journal Of Pain. 2014; 28(1):18.
-
Gupta K, Rastogi B, Gupta P, Singh I, Bansal M, Tyagi V. Intrathecal nalbuphine versus intrathecal fentanyl as adjuvant to 0.5% hyperbaric bupivacaine for orthopaedic surgery of lower limbs under subarachnoid block: A comparative evaluation. Indian Journal of Pain. 2016; 30(2):90-95.
-
Shakooh S, BhonsleP. . Intrathecal Nalbuphine: An Effective Adjuvant for Post OperativeAnalgesia. Innovative Journal of Medical and Health Sciences. 2014;4(2):79-82.
-
ThoteJ.R,LomateP.ComparisonAmongIntrathecalFentanylAndNalbuphineInCombinationWithBupivacaineAndPlainBupivacaineForLowerLimbSurgeries.InternationalJournalOfRecentTrendsInScienceAndTechnology.March2015;14(2):361-366
-
NazS,ShuklaU.AComparativeStudyOfAnalgesicEffectOfIntrathecalNalbuphineAndFentanylAsAdjuvantInLowerLimbOrthopaedicSurgery.JClinDiagnRes.2017;11(7):25-28.
-
T Padma, K Mydhili. A Comparative Study ofPost Operative Analgesia After Spinal Nalbuphine with Bupivacaine and Spinal Bupivacaine for Lower Limb Surgeries. Journal of Evidence Based Medicine and Healthcare. 2015;2(38):6105- 6109.
-
SinghH,YangJ,ThorntonK,GieseckeA.Intrathecalfentanylprolongssensorybupivacainespinalblock.CanadianJournalofAnaesthesia.1995;42(11):987-991
-
Thote J. R, Lomate P. Comparison among Intrathecal Fentanyl and Nalbuphine In Combination with Bupivacaine and Plain Bupivacaine for Lower Limb Surgeries. International Journal of Recent Trends in Science and Technology. March 2015 ;14(2):361-366
-
R Manjula, G V Chaithra. Comparitive Study of Bupivacaine with Nalbuphine and Bupivacaine alone for Post-Operative Analgesia in SubArachniod Block for Lower Limb SurgeriesProspectiveRandomised Study. J AnestandIntenCare Med. 2017;2(2):555-581
-
Gupta K, Gupta A, Neeraj . Efficiency of nalbuphine as an adjuvant to bupivancainein lower limb orthopaedic surgery-a prospective study.International Journal ofResearch in Medical Sciences. 2017; 5(2):623-626.
.
.
 Home
Home This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.