 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 11 Issue 1 -July 2019
Effect of oral premedication of melatonin on anxiety and sedation in preoperative period before induction of general Anaesthesia
K Udaya Bhaskar1, K V Suma2*, Tanuja3, K V Srinivasan4
1Assistant Professor, 3Post Graduate, 4Professor, Department of Anesthesiology, PES Institute of Medical Sciences and Research. Kuppam. 2Associate Professor, Department of Anesthesiology, JJM Medical College, Davanagere.
Abstract Background: Preoperative anxiety can cause undesirable effects on both induction of anesthesia and maintenance and also recovery. Benzodiazapenes like midazolam are the commonly used drugs for allaying anxiety but are associated with deep sedation and impaired cognition. Melatonin a naturally occurring neuro hormone in the body is shown to have anxiolysis and sedation without causing deep sedation and impairment of cognition. Aims and objectives: To evaluate the effects of melatonin in prevention of anxiety and producing sedation in the preoperative period. Methods: Sixty ASA physical status I and II patients of both sex scheduled for surgery under general anesthesia aged18-55 years were divided in to two groups. In Group M 0.2 mg/kg oral melatonin was given 60 minutes before induction and in Group C placebo was given ..VAS anxiety score ,sedation score and orientation score, along with heart rate and mean arterial pressure were recorded before administering the study drugs and at 0,15,30 45,60 minutes following administration. Adverse effects of melatonin if any were noted. Results: In group M patients were less anxious and had good sedation than in the group C which was significant at 15,30,45 and 60 minutes following the administration of premedication.(p<0.01). A significant decrease in both the heart rate and MAP was also seen in the group. Conclusion: Melatonin (0.2mg/kg) oral reduces anxiety and causes sedation without any side effects preoperatively Key words; anxiety, melatonin, orientation, preoperative, sedation
INTRODUCTION During the preoperative period anxiety is commonly seen in patients posted for surgery1. An unpleasant state of tension or an uneasy feeling because of patients concern regarding the disease, hospital admission, anesthesia and surgery is described as preoperative anxiety.2 It can lead to sympathetic stimulation and in some cases may lead to patient deferring surgery. may cause patients to avoid planned surgery.3 High levels of preoperative anxiety can have unfavorable effects on induction as well as maintenance of anaesthesia and lead to a delayed recovery from anaesthesia due to higher doses of induction agents and post operative analgesic drugs.4 An important goal in optimal anaesthetic management is to reduce the anxiety and this can be accomplished by good premedication.5 Preoperative anxiety can be reduced with certain pharmacological interventions. Benzodiazepines like midazolam is commonly used as a premedication to decrease the levels of anxiety. It has disadvantages like paradoxical reactions, variable bioavalibity, can interact with opioids and lead to a delay in discharge from the post anaesthesia care unit.6 A naturally occurring neurohormone Melatonin(N-acetyl-5-methoxy tryptamine) is secreted in the human body by the pineal gland.7,8,9 Studies have shown that decrease in pre operative anxiety and sedation can be caused by melatonin without impairing orientation ,psychomotor skills and cognition which in turn improve the quality of recovery.10 It is a novel hypnotic with anaesthetic sparing effect and a wide safety margin[11]' in children a dose of 0.4 mg/kg has been used safely. As a result we designed this study to evaluate the effects of premedication with melatonin on preoperative anxiety and sedation.
MATERIALS AND METHODS Ethical committee clearance from the institute and patient consent after explaining about the study was obtained. Patients included in study were those undergoing surgeries under general anesthesia for general surgical procedures, ENT surgeries and orthopedic procedures in the age group of 18 to 55 year, both male and female belonging to ASA Physical status I and II. A minimum sample size of 20 in each group was needed with the power of study at 80%, and alpha error(confidence intervals)at 95%. we included 30 patients in each group in order to make up for possible drop outs and also for better validation of results. It was a prospective randomized control study. Pregnant and lactating woman, patients who had psychiatric disorders and taking antipsychotic medications, those with sleep disorders and language or communication difficulties were excluded from the study. Patients were divided in to two groups. Group M: Melatonin group in which 0.02mg/kg melatonin was administered by oral route in the form melatonin tablets [Meloset 3 mg]sixty minutes before surgery. Group C:Control group in which multivitamin tablet was administered by oral route[Becosule tablet] 60 minutes before surgery
RESULTS Number of patients, age, sex ratio, weight and duration of surgery were not different between the groups.
Table 1: Demographics
Visual anxiety score The Mean VAS anxiety scores before administration of premedication in melatonin group and control group were and 5.98±1.10 and 5.67±0.82 (P=0.172) without any significant difference. At 0 min the VAS anxiety score was 5.98±1.10 in the melatonin group and 5.67±0.82 in the control group (p=0.172.) being non significant. It was3.63±0.9 in the melatonin group and 4.83±0.71 in the placebo group(p,0.001) at 15 minutes after premedication and was strongly significant. At 30,45 and 60 minutes following premedication the VAS scores for anxiety were significantly lower melatonin group(2.43±0.93, 1.30±1.09, 0.45±0.81 respectively in melatonin group and4.80±0.56, 4.70±0.56, 4.70±0.65 in the control group p<0.01 at all the intervals.
Table 2: Visual anxiety score
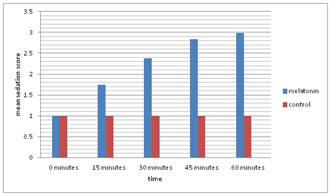
Sedation score: All the patients had a sedation score of 1 in both the groups before administration of study drug. At 15 minutes twelve patients had a sedation score 1,sixteen had a score of 2 and two had a score of 3 in the melatonin group while in the control group all the thirty patients were awake with a sedation score of 1(p<0.01) and strongly significant .At 30 minutes after premedication two patients had a sedation score of 1,eighteen patients had a score of 2 and ten patients had a score of 3 and in the control group all the thirty patients had a sedation score of 1(p0.01) and strongly significant. Forty-five minutes after premedication eight patients in melatonin group had a sedation score of 2 and twenty two patients had a score of 3 but in the control group all the patients had a score of 1 (<,0.01) and being strongly significant. At 60 minutes after premedication two patients in the melatonin group had a sedation score of 2 and twenty eight patients had a score of 3 while in the control group all the thirty patients were awake with a score of 1(p<0.01) and highly significant .None of the patients had a sedation score of 4 in both the groups . Figure 1:Mean sedation score Figure 2: Orientation scores Orientation scores Patients in both the groups had orientation score of 2 at baseline,0,15,30,45,60 minutes after administering the study drug. Heart rate The mean baseline heart rates in both the groups were similar. In melatonin group at 15 minutes a significant decrease was seen(P=0.041)and at 30,45,60 minutes the heart rate decreased in a strongly significant manner (P<0.001) when compared to the control group.
Table 3: Heart rate
MEAN ARTERIAL PRESSURE[ MAP] There was no difference in the mean arterial pressure before administration of the study drugs between the groups .A significant fall in MAP was seen in the melatonin group after 15 minutes of drug administration with a maximal fall at 60 minutes( p<0.01). There was a fall in control group but was not significant from the basal value. DISCUSSION Unfavourable effects of preoperative anxiety is seen on both induction as well as maintenance of anaesthesia and it can also affect the recovery from anaesthesia. Good anaesthetic management necessitates the use of premedication in order to provide anxiolysis. Currently used drugs for premedication to reduce anxiety are effective, but certain undesirable effects and complications can be seen with them. Alternative medications with increased margin of safety yet producing a similar degree of anxiolysis is desirable. Sedative and hypnotic properties of melatonin are seen when administered exogenously. Based on this a postulation was made that melatonin on oral administration could be a potent and safe drug for anxiolysis and sedation.16,17 The previous studies done have yielded mixed results, in some melatonin producing good anxiolysis[18,12] while in others effective anxiolysis was not seen.[19,20]Therefore we conducted a study to evaluate the effectiveness of oral melatonin administered 60 minutes before surgery in producing anxiolysis and sedation in adults when compared with placebo. We used 0.2mg/kg oral dose of melatonin as previous studies done by Naguib et al21 found this to be effective. Exogenous melatonin has a peak effect between 60-150 minutes. So we administered the drug 60 minutes before the surgery. Number of patients, age, sex ratio ,weight and duration of surgery were not different between the group .The mean VAS anxiety score was significantly less in the melatonin group at 15,30,45 and 60 minutes after premedication being 3.63±0.92,.43±0.931.,30±1.090.,45±0.81 respectively while the scores in the placebo group were 4.83±0.71, 4.80±0.56, 4.70±0.56,4.70±0.65 at the above said time intervals and was strongly significant.(p<0.01). . and Naguib et al[16], Caumo et al [15], Mowafi et al21, in their studies found melatonin to produce good anxiolysis in relation to placebo similar to our findings .Anxiolysis seems to be due to activation of melatonin receptor and gamma-aminobutyric acid transmission.22 Capuzzo et al [19][ did not find a significant reduction in anxiety in the melatonin group compared to control .This could be due to a lesser dose of melatonin used by them(maximum 10mg in contrast to 0.2mg/kg used in our study)..The mean sedation score in the melatonin group was1.75±0.54, 2.38±0.59, 2.83±0.38, 2.98±0.16 at 15,30,45 and 60 minutes respectively and in the placebo group it remained at1.00±0.00 at all the specified time intervals. In a study done by Naguib et al [12] comparing midazolam ,melatonin and placebo highest sedation was seen in midazolam group than the melatonin group and was significant .however the sedation seen in melatonin group was significantly higher than in the placebo group .Acil et al [24] also found a significant difference in the level of sedation when comparing placebo and melatonin .The sedation seen in the melatonin group is better than the placebo group and not as deep as in midazolam group reducing the need for preoperative monitoring ..This correlates with our study. With respect to orientation in two studies, Naguib et al and and Acil et al found the orientation scores to be similar between the melatonin and placebo group .In our study also the orientation scores remained at two at all the time intervals in both the groups and is similar to the above studies .A significant fall in heart rate and MAP was seen in melatonin group at 15,30,45 and 60 minutes after premedication while not much change was seen in the control group .This is because melatonin by reducing anxiety and producing sedation led to a significant reduction in heart rate and MAP. No side effects of melatonin were seen in our study.
CONCLUSION We conclude that oral melatonin produces a significant anxiolysis and sedation without affecting orientation when given as a premedicant in the dose of 0.2mg/kg (tablet) sixty minutes before surgery without producing any side effects. Further studies are needed to evaluate different doses and formulations of melatonin.
REFERENCES
. |
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.