 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 11 Issue 3 -September 2019
Anaesthetic challenges in a patient with Glucose-6-Phosphate dehydrogenase deficiency: A case study
Megha Wadhwani1*, Joseph George Tharion2, Rajat Gupta3
1,3Senior Resident,2Junior Resident, Department of Anaesthesia, VMMC and Safdurjung Hospital, Delhi, INDIA. Email: megha_doctr1488@yahoo.in
Abstract The management of a patient with Glucose-6-Phosphate Dehydrogenase (G6PD) deficiency, involves careful pre-operative assessment, including a thorough work-up, optimisation of haematocrit, and being prepared for transfusion of blood. For the intra-operative period, careful planning is required to make sure that all drugs which are known to precipitate hemolysis either directly or indirectly are avoided. Similarly, post-operative care involves avoiding contra-indicated drugs and precautions against infections or similarly stressful situations. We present the perioperative management of a patient with G6PD, scheduled to undergo a ureteric re-implantation for chronic hydroureteronephrosis and vesico-ureteric reflux. All the necessary factors were accounted for, the case proceeded smoothly, and the patient was discharged uneventfully. Key Words: haemolytic anaemia, X-linked recessive, males, enzyme deficiency, oxidative stress.
INTRODUCTION Glucose-6-Phosphate Dehydrogenase deficiency is an inherited X-linked enzymatic disorder that results in Coombs-positive hemolytic anemia.1 G6PD catalyses the first step in the pentose phosphate pathway, that is responsible for generating NADPH, which is important in preventing and reversing oxidative damage to cellular components. 2 In a deficient state, most body tissues have other mechanisms of combating oxidative stress, but for red blood cells (RBCs), this is the only pathway which via NADPH maintains Glutathione in its reduced state, as an anti-oxidant.11 Thus when these patients are exposed to oxidative stress such as the intake of certain drugs, fava beans, or infections, there is resultant haemolytic anaemia.2 In peri-operative medicine, it is important to ensure that the patient is not already in a state of hemolysis and anemia, and secondly, the drugs administered should be carefully planned so as to not use any medication with either known or theoretical risk of causing oxidative stress, inadvertently or otherwise.
CASE REPORT A 2 year old boy presented with antenatally detected left sided hydroureteronephrosis, and grade 5 vesico-ureteric reflux to the left kidney. He was evaluated by the paediatric surgical team and a left open ureteric re-implantation was planned. On pre-operative evaluation of the patient, it was discovered that he had prior hospital admissions for recurrent infections. He had history of anaemia, and a neonatal diagnosis of G6PD deficiency. As described by the parents, during the 30th week of the mother’s first pregnancy, a routine antenatal scan showed left sided dilated pelvicalyceal system, no other abnormalities. They were advised to do a close follow up post-natally. He was delivered by lower segmental caesarean section (LSCS) at 39 weeks of gestation for the indication of failure of labour to progress. He had a birth weight of 2.483 kilograms and no intrapartum complications. The baby cried immediately after birth, passed urine and meconium, was normotensive and was tolerating breastfeeds well. There was no history of jaundice, scleral icterus,dark urine, hepatosplenomegaly or anaemia. A routine newborn screening assay revealed that he had G6PD deficiency, with enzyme levels of 0.1Units/gm of Haemoglobin. He was discharged, and subsequently received all immunizations as per the national schedule.By 7 months of age, he developed high grade fever, for which he required admission and antibiotics, and took a course of 20 days. There were repeated similar episodes over the next few months, and eventually they were advised to get further investigations at a higher centre. An ultrasound scan done at a tertiary care centre revealed left sided hydroureteronephrosis, and grade 5 vesico-ureteric reflux to the left kidney. He was also found to have severe microcytic hypochromic anaemia, with a haemoglobin of 6.9gm%, with low iron stores. Liver function tests showed a mildly elevated aspartate transaminase (AST) 57 Units/L. He was normotensive throughout. Renal function tests were normal, and urinalysis and urine and blood cultures were negative. Echocardiogram was normal. A 99m-Tc DMSA Renal scan showed a small hydronephrotic left kidney with relative left renal function of only 9.4%, and a well functioning right kidney. A micturating cystourethrogram (MCU) showed a left sided grade 5 vesico-ureteric reflux. His glomerular filtration rate (GFR) was 94ml/minute/1.73m2 . He was started on iron supplements orally, and was advised a surgical corrective procedure - ureteric re-implantation.The course of the surgery and the anaesthetic plan was discussed in detail with the family, and all the standard risks as well as those specific to his disease process such as acute and delayed hemolytic anemia, avoidance of contra-indicated drugs, and ICU admission were explained. An informed consent was taken for all of the above. Routine pre-operative baseline investigations including electrolytes were done, all of which were within normal limits. On the day of surgery, the patient, weighing 10 kgs, was brought into the operation theatre and connected to monitors. A 24 Gauge peripheral line was in-situ in the right hand. The child was given inhalational induction with sevoflurane in oxygen. 2 mic/kg of Fentanyl was given intravenously. After a successfully confirming that mask ventilation was possible, 0.5mg/kg of Atracurium was given. He was ventilated for 3 minutes with a pressure of 10cm with oxygen and sevoflurane. He was then intubated with a 4.0 sized uncuffed portex endotracheal tube, using a Macintosh laryngoscope size 2 blade. Tube position was confirmed by auscultation and EtCO2 monitoring. Outcome and Follow-up Post operatively he was pain and nausea/vomiting free, awake and conscious while in the recovery unit, and was discharged to the ward after a period of monitoring. His condition continued to improve in the ward, with no evidence of haemolysis. He was discharged on the 12th postoperative day.
DISCUSSION G6PD deficiency is the most commonly occurring enzyme deficit, affecting approximately 400 million people worldwide. 3 The prevalence in India is 3%. 4 The geographical distribution correlates with areas endemic to Malaria, as G6PD deficiency imparts increased resistance to plasmodium falciparum, which cannot tolerate the increased levels of oxidative stress. The WHO grading divides patients into 5 classes based on the enzyme level, class I being the most severe, and more commonly associated with chronic haemolytic anaemia. 5 Over 140 different genetic variants of the disorder have been described. 3For the majority of individuals, the condition is benign, with no baseline haemolysis. Only when exposed to certain triggers, such as medications, food and infections does acute hemolytic anaemia present. 6G6PD deficiency was first brought to light in 1926, when haemolysis due to antimalarials, specifically 6-methoxy-8-aminoquinoline drugs was being investigated.7 However it would be another 30 years before the mechanisms would be understood. This was largely due to the labours of renowned scientists such as Warburg, Embden and Meyerhof, who worked out the biochemical pathways of red cell utilisation of glucose. The clinical investigations specific to the investigation into haemolysis was done on prisoner volunteers from the Illinois State Penitentiary, US, prior to the establishment of Institutional Review Boards (IRB). 8G6PD is a key enzyme in the rate limiting step of the Pentose Phosphate Pathway (PPP), in which glucose is converted to a 5-carbon form ribose-5-phosphate. As this takes place, nicotinamide adenine dinucleotide phosphate (NADP+) is converted to its reduced form NADPH. 9 This then becomes the reducing power of the cell, by maintain Glutathione in its reduced form. Reduced Glutathione has potent anti-oxidant activity, and protects the cell from free radical and oxidative damage.10 Whilst other cells have multiple metabolic pathways to generate the reductive agent NADPH, for red blood cells the PPP is the only modus. 11 Hence when disturbed, the red cells are relatively unprotected, and are prone to haemolysis when challenged with oxidative stress. This can have multiple causes, such as infections, drug intake, certain foods such as fava beans, metabolic derangements like diabetic ketoacidosis and even surgical stress. The haemoglobin undergoes oxidative denaturation and forms clumped precipitates that can be identified on a peripheral smear as Heinz bodies. 3Prevention is the cornerstone in the management of a patient with G6PD coming for surgery. An adequate pre-operative work up should identify that the patient is not actively in haemolysis, as shown by clinical features such as jaundice, pallor and high coloured urine in children, and fatigue and splenomegaly in adults. Laboratory tests include a complete blood count, liver functions tests such as levels of bilirubin, lactate dehydrogenase enzyme, serum aspartate and alanine transaminase enzyme, reticulocyte count, haptoglobin, urinalysis, Coomb’s test and peripheral blood smear for signs of haemolysis. 3,9,16 Elective cases need to be treated and optimised with supportive care and haematinics in mild cases, and transfusions if severe. In a patient that is deemed fit for surgery, scrupulous pre-operative planning is required. Drugs that are known to precipitate hemolysis in G6PD patients have to strictly be avoided, as listed in Table 1.3,12,13 Table 1:
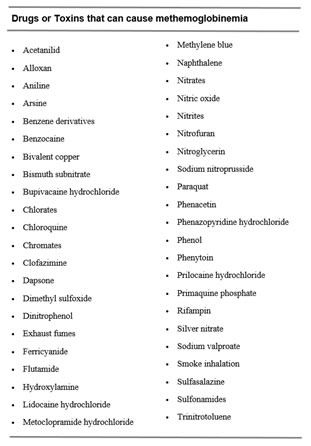
Another seemingly unrelated, yet important concern is methaemoglobinemia. This is a condition where the Ferrous (Fe2+) ion in the haeme of haemoglobin is oxidized to Ferric (Fe3+) state. The treatment of choice for this disease process is intravenous methylene blue, which is reduced by NADPH dependant enzymes to leucomethylene blue, which then reduced the altered Iron back to its Ferrous form. However in patients with G6PD deficiency, NADPH is lacking, and the methylene blue remains unreduced. This itself causes oxidative damage, precipitating severe hemolysis on top of an already ongoing disease process, which can result in death. Alternative therapies must be instituted in these cases, such as hyperbaric oxygen therapy and blood transfusions. This leads us to another important planning point- that drugs that may cause methaemoglobinemia must also be avoided. 9 This includes some local anaesthetics such as benzocaine, lidocaine, articaine, bupivacaine and prilocaine, silver nitrate, phenytoin, and others as listed in Table 2. (14)
There has not yet been significant research into the effect of anaesthetic agents in G6PD patients. In vitro studies showed that isoflurane, sevoflurane, diazepam and midazolam had an inhibitory effect on G6PD activity, whereas halothane, ketamine and prilocaine had none.15 However there are no documented cases of haemolysis caused by these drugs in-vivo.10 Intra-operative hemolytic crisis is hard to detect, as clinical features such as hypotension can be attributed to surgical or anaesthetic causes. However the course of surgery has to be monitored and planned, taking care avoiding events such as hypoxia, ischaemia (from tourniquet use), inadequate analgesia, pre-operative anxiety or anything else that can cause oxidative stress.17 The post-operative period also requires vigilant monitoring, as a haemolytic crisis arising from drug administration manifests in 24 - 72 hours, and worsening anemia for 7 days. 3 Hence the signs and symptoms should be watched for in the ward, or if discharged early, the caretaker and patient must be aware of the danger signs. Laboratory investigations mentioned earlier for signs of hemolysis can be done if there is any suspicion of the same. Treatment is mostly supportive, leading up to a blood transfusion if required.10 In our patient, the known enzyme level done at birth was <0.1 Units, thus falling in WHO class I severe category. There was no history of features of chronic hemolytic anemia, only that of acute episodes. Nevertheless, a high degree of caution was required. Pre-operative examination showed no features of haemolysis, and his laboratory investigations were within normal limits, with a haemoglobin of 12.7 gm/dl. As the patient was a child coming for an open ureteric re-implantation, general anaesthesia was planned. Only drugs that are known to be safe and/or have no reported cases of haemolysis were used. Induction was with sevoflurane, fentanyl and atracurium. Local anaesthesia both in the form of caudal and post-op surgical incision infiltration was avoided, as there is a risk of methaemoglobinemia with the same, which can result in disproportionately severe side effects. Nitrous oxide was used for intra-operative anaesthesia, and morphine was given for both intra-operative and post-operative anaesthesia. Acetaminophen was avoided as it is contraindicated in class 1 G6PD deficiency. Adequate depth of anaesthesia, insulation of exposed parts, temperature monitoring and appropriate warm fluids were used to maintain homeostatic conditions throughout. There was minimal blood loss and the surgery went according to plan. His post-operative period was uneventful. There were no clinical signs of haemolysis, and a complete blood count did not show any anaemia, hence he was not investigated further. He came for follow-up in OPD after a month, with good signs of improvement and no signs of late haemolysis.
CONCLUSION G6PD Deficiency is a rare disease that presents as a spectrum, and inattentive management is associated with largely preventable complications that significantly worsen post up outcome, hence a high degree of vigilance is required when these patients require the administration of Anaesthesia. An optimal pre-operative workup, and meticulous planning of anaesthetic medications, along with a detailed discussion with the patient and family will ensure that the best possible care is given. In our case, giving regard to all known and reported risk factors in G6PD patients resulted in a successful procedure, followed by an unventful post-operative period and a timely discharge from the hospital. As more such cases are reported in literature over time, we hope that an evidence based protocol can eventually arise to benefit all patients with G6PD that present for surgery.
REFERENCES
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.