 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 12 Issue 2 -November 2019
Comparative study of local versus spinal anaesthesia in long standing open inguinal hernia in patients of south Karnataka
N S Shreesha
Consultant/ DNB Teacher, General hospital Jaynagar, 4th T Block, Bangalore-560041. Email: shreesha1956@gmail.com
Abstract Background: Hernias are the quite common disadvantageous for erect posture in human beings. Inguinal hernia occurs 15-20% due to intra-abdominal pressure against gravity, hence anterior abdominal muscles are antigravity muscles and more prone for inguinal, hernia. The common Anaesthetic techniques for inguinal hernia repair are local anesthesia, spinal or general anesthesia. Hence attempt was made to compare the pros and cons of both methods males. Method: Out 66 adults aged between 32 to 55 years were studied. The patients were classified into 2 groups A group(Local anesthesia) and group B(spinal anesthesia 33 patients in each group. The patients with unilateral, reducable, indirect, longstanding (chronic) inguinal hernia patients were studied, Routine Blood examination, RBS, chest-x-ray, ECG was done to certify the feasibility. Results: The duration of surgery was more in local anesthetic group A, as compared to B group but VAS scale study was more in group A(local) anesthesia. Post-surgical complications like wound infections, re-admission, urinary retention post –operative hydrocele were more significant in group B(spinal anesthesia) Conclusion: For chronic or long standing inguinal hernia spinal anesthesia is ideal because of shorter duration of surgery and least pain. `Key words: Local anesthesia, spinal (general) Anesthesia, VAS, recurrence.
INTRODUCTION Inguinal hernias are the most common problems in 10-12% of Indian population. It is one of the most disadvantages of erect posture. Anaesthetic procedures commonly performed world-wide, can be spinal/ epidural anesthesia and local anesthesia, depending upon the varieties of factorsviz, surgeons wish, patients acceptance, safety, feasibility and cost1’2. But patients’ safety should be the paramount importance in choosing type of anesthesia. The studies comparing the recovery profiles of local, general and regional anesthesia show that, local anesthesia is ideal for day care surgery3. Local anesthesia provides increased safety for patients, better post-operative pain control, and shorter recovery period with least duration of hospital stay and reduced cost. Localanesthesia is widely acceptable because of safer technique for inguinal hernia surgery4. Hence attempt was made to evaluate the duration of surgery pain tolerance, post operative complication in both groups.
MATERIAL AND METHODS 66 (sixty six) patients aged between 32 to 55 years old males regularly visiting to surgery department of General hospital Jaynagar, 4thT Block, Bangalore-560041 were studied Inclusive criteria- The male patients having single sided reducable, indirect, long standing, chronic inguinal hernia, ASI grade-I and II were selected for the study. Exclusion criteria– The patients with recurrent, bilateral irreducible, strangulated, incarcerated, obstructed hernia, immune-comprised patients were excluded from the study. Method-After admission routine blood examinations, like Hb%, CBC, RBS, renal function test, chest-x-ray, ECG, were done. The sixty six (66) patients divided in two group A and B by lottery system. A group (33) patient was subjected to inguinal hernia mesh repair under local anesthesia. Group B were subjected to inguinal hernia mesh repair under spinal anesthesia. In group A patients 0.25% Bupivacaine between 20 -30 ml was administered . A skin weal was raised, 2.5 cm from the iliac crest along the line joining anterior superior iliac spinal to umbilicus. A needle was then passed through this to strike the inner surface of ileum just below the crest. 5ml of the solution was deposited as needle was slowly withdrawn. The injection was repeated with needle reinserted at a slightly steeper angle and 8ml solution was deposited. Second point of block was 2cm above the mid-inguinal point. The needle was inserted perpendicularly until it pierced the aponeurosis of external oblique. 5ml solution was deposited at this depth and 5ml as needle was withdrawn over 2cm. Next a weal was raised over the pubic tubercle and subperiostealinjection of 5ml of solution was made. The block was completed by subcutaneous infiltration along the line of surgical incision and 5ml of solution was deposited. In group B patients spinalanesthesia was given by using Bupivacaine 0.5% heavy. Under strict aseptic precautions subarachnoid block was performed using a mid-line lumbar approach with patient in sitting or lateral position with25 gauge spinal needle in L3-L4 inter space 3ml of 0.5% Bupivacaine was injectedinto sub-arachnoid space after getting free flow of cerebrospinal fluid(CSF).Patients was turned supine. In case of inadequate or no effect of local or spinal, anesthesia was converted into general and such patients was not included in the present study. Tension free Liechtensteinhernioplasty was done in both groups. Material used for hernioplasty was polypropylene prosthetic mesh with dimension of 15X7cm. After the surgery post-operative complicationsand recurrence were noted in both groups. Total duration of study was from December 2017 to may 2019. Statistical analysis- The duration of surgery, Intra operative pain, post-operation complication, visual analogue scale-(VAS) was applied to both groups.No pain VAS-0, mild pain VAS 1,2,3, moderate VAS=4-6, sever VAS>7 were compared in both group with percentage.
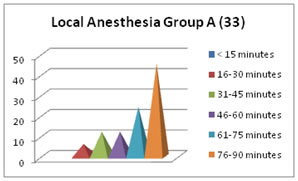
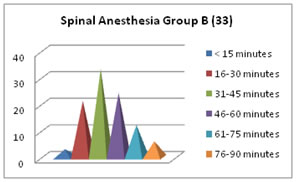
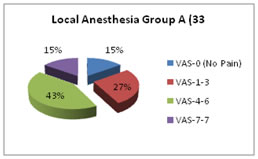
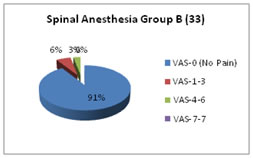
OBSERVATION AND RESULTS Table-1–Comparative study of duration of surgery in both groups. In group B1(3%) had surgery less than 15 minutes (<15 minutes). In group A 2(6.06%) had surgery less than 15 minutes.In group B-7 patients(21.2%) duration of operation was between 16-30 minutes andgroup A-4 (12.1%), in group B 11(33.3%) had duration of surgery was31-45 minutes. Group A-4 (12.1%) and group B 8(24.2%) The duration of surgery was 46-60 minutes. In group A 15(45.4%) and group B2 patients(6.06%) had duration of surgery was 76-90 minutes. Table-2–Comparison of post-operative (VAS) in both groups- A, group had VAS-0 were 5(15.5%), group B had 30 (90.9%) had VAS-0. In group A VAS 1 to 3 was 9(27.2%) and in group B-2 (6.06%). In group A VAS-4 to 6 was 14(42.4%)and in group B-1 (3.03%). In group A VAS>7 were 5(15.1%) and in group A VAS>7 were 5(15.1%) and in group B were zero. Table-3- post- operative complication In group B- 5(15%) retention of urine, In group A wound infection was 2(6.06%)and group B 3(9.09%), Readmission Group B only 1(3.03%) post-operative hydrocele 1(3.03%) in group A, 2(6.03%) in group B
Table 1: (No of patients 66)Comparative study of duration of surgery in both groups
Table 2: (No of patients 66)Comparative study of intra-operative pain (NAS) in both groups with percentage
Table-3: (No of patients 66) Comparison of post- surgical complication in both groups
DISCUSSION In the present comparative study of local versus spinal anesthesia in long standing inguinal hernia in patients of south Karnataka population. In the comparison of duration of surgery- group B had 1(3%) more less than 15 minutes, In group A 2(6%) group B had 7(21.2%) had duration of 16-30 minutes. In group A-4 (12%) in group B11(33.3%) had duration of 31-45 minutes, In group A-(12.1%)and group B 8(24.2%) had duration of surgery was 46-60 minutes. In group A 15(45.4%) and group B2(6.06%) had duration of surgery was 76-90 minutes (Table-1). In comparison of post-operative (VAS) in both groups- A, group had VAS-0 were 5(15.5%), Group B had 30 (90.9%) had VAS-0. In group A VAS 1 to 3 was 9(27.2%) and in group B-2 (6.06%). In group A VAS-4 to 6 was 14(42.4%) and in group B-1 (3.03%). In group A VAS>7 were 5(15.1%) and in group A VAS >7 were 5(15.1%) and in group B were zero.(Table-2). post- operative complication In group B- 5(15%) retention of urine, In group A wound infection was 2(6.06%)and group B 3(9.09%), Readmission B only 1(3.03%) post-operative hydrocele 1(3.03%) in group A, 2(6.03%) in group B (Table-3). These finding were more or less in the agreement with previous studies5’6’7. In the present study, the majority of the inguinal hernias were right sided. It is due to later descent of right testes and high incidence of patent processes vaginalison right side8. It was observed that VAS analogue was more significant in group A (local anaesthesia) as inguinal region includes, the inguinal canal, the spermatic cord and the surrounding soft tissue structures.It receives its sensory innervations from three nerves- iIiohypogastricnerve, Ilio-inguinal nerve and genitofemoral nerve. Iliohypogastric nerve (T12-L1) passes through the external inguinal ring, usually closely associated with spermatic cord. The genito femoral nerve (L1-L2) also supplies spermatic cord structures and anterior scrotum. Its genital branch supplies skin and sub-cutaneous tissues of the femoral trianglevia- femoral branch. In the local anesthesia (Group A) patients it could have difficulty to provide blockage of all these nerves9. Hence the surgery by local anesthesia was more painful as compare to spinal unaesthetic surgery. It was also reported that, during local anesthesia some sedation was necessary to overcome the pain10. It was also reported inguinal hernia surgery by local anesthesia in older patients have higher rates inguinal hernia repair11. Hence in elder patients long standing or chronic inguinal hernia, spinal anesthesia is recommended to avoid repeated inguinal repair and pain during surgery.
SUMMARY AND CONCLUSION In the present comparative study of spinal anesthesia versus local anesthesia in long standing open inguinal hernia repair Spinal anesthesia was proved comfortable, easier and painless. Although the Lichtenstein tension free hernioplasty under local anesthesia is used without any morbidity.But spinal anaesthesia was proved best in chronic or long standing ,unilateral Hernia and in elderly patients. REFERENCES
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.