 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 12 Issue 3 -December 2019
Evaluating the additive effect of dexmedetomidine with levobupivacaine in axillary brachial plexus blockade
Anandha Lakshmi D1, Kamalakannan M2*
1Assistant Professor, 2Associate Professor, Department of Anaesthesiology, Karpagam Faculty of Medical Sciences and Research, Coimbatore - 641 021 Tamil Nadu, INDIA. Email: kamal97@gmail.com
Abstract Anesthesia for furthest point and shoulder medical procedure can be accomplished by nerve bar of the brachial plexus. The utilization of levobupivacaine in brachial plexus squares appears to be encouraging thinking about the lower danger and the need of enormous volumes. In this paper is used to evaluate the additive effect of dexmedetomidine with levobupivacaine in axillary brachial plexus blockade. Brachial plexus blockade, root of brachial plexus by the association of ventral rami of lower four cervical nerves and first thoracic nerve (T1) with incessant commitments from C4 or T2. The dexmedetomidine may cause sedation without respiratory wretchedness and unfriendly impacts like hypotension, bradycardia might be seen with expanded dose. Key Word: Brachial Plexus, Levobupivacaine, Dexmedetomidine, Anesthesia
INTRODUCTION Anesthesia for furthest point and shoulder medical procedure can be accomplished by nerve bar of the brachial plexus. Bupivacane is a racemic blend made out of 2 enantiomers, dextro-bupivacaine and levobupivacaine. It is frequently utilized as a nearby soporific for fringe nerve squares since it has a more drawn out term of activity and starts tactile square than engine square1. In clinical use, it was noticed that utilizing this blend of bupivacaine causes cardiovascular and neurological poisonous impacts. This dangerous impact is predominantly because of the nearness of dextro – bupivacaine enantiomer. This incited examiners to grow new neighborhood soporific operators which comprises all properties like racemic blend of bupivacaine without the harmful impacts. Levobupivacaine, the S-enantiomer of bupivacaine is the more up to date nearby sedative medication brought into clinical practice. This enantiomer has a similar sedative movement as bupivacaine however with lesser heart and neural poisonous impacts. This medication has been demonstrated to be protected and successful for epidural and intrathecal anesthesia and for the fringe nerve blocks.2 Anyway relatively few examinations have been directed contrasting the adequacy of this medication and Dexmedetomidine. Dexmedetomidine is an exceptionally specific alpha 2 agonist, with 1600-overlay more prominent selectivity for alpha 2 than the alpha1 receptor. It has as of late been affirmed for brief sedation under 24 hours in escalated care units.3 Assistant bronchial plexus square is generally utilized in numerous upper appendage techniques. We can browse a few approaches, for example, the huge volume of nearby sedatives required for its shared factor, the examination with neuroaxial volume, and the decision of neighborhood anesthesia. The utilization of levobupivacaine in brachial plexus squares appears to be encouraging thinking about the lower danger and the need of enormous volumes. In any case, the probability of unsuitable engine bar, both in neuroaxial and brachial plexus squares, presently can't seem to be discredited.4
AIM OF THE STUDYThe aim of this study is to evaluate the additive effect of dexmedetomidine with levobupivacaine in axillary brachial plexus blockade.
MATERIALS AND METHODS Study structure: This is a planned, twofold blinded, randomized clinical interventional trail. This investigation was done at Government Stanley Medical school clinic, Chennai during the time of April 2013 to December 2013. In the wake of getting endorsement from the Institutional Ethical Committee of the Stanley Medical College, Chennai-1, a pilot study was done to figure the example size. The pilot study got the estimation of mean and standard deviation of Duration of Sensory square time of Group-1 (11.78 ± 3.65) and Group-II (13.23 ± 3.95). Statistical Analysis: The information were investigated utilizing SPSS (Statistical Package for Social Science) Ver. 16.01. The information gathered were scored and broke down, Continues factors were introduced as methods with Standard deviation (SD) and all out factors were displayed as recurrence and rates. Understudy t-test was utilized for testing the criticalness of the considerable number of factors (Mean and SD) in both the gathering. Chi-square test was utilized to look at extents. All the Statistical outcomes were viewed as critical at P esteem < 0.05. 120 patients of ASA I physical status who got conceded for upper appendage (lower arm and hand) surgeries were contemplated. They are partitioned into two gatherings of 60 each. Gathering ONE – 30 ml of levo bupivacaine {0.5%} with ordinary saline{1ml} Group TWO – 30 ml of levo bupivacaine {0.5%} with dexmedetomidine {100mcg} Incorporation criteria: All assented patients matured somewhere in the range of 18 and 60 years of the two sexual orientations having a place with ASA I and ASA II, weighing between 50kg – 70 kgs posted for Elective lower arm and hand medical procedures. Exclusion Criteria: Patients receiving adrenoreceptor agonist and antagonist therapy.
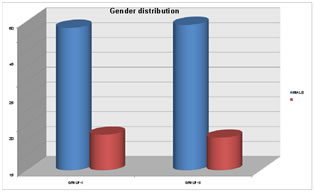
OBSERVATION AND RESULTS Statistical Tools: The data gathered with respect to all the chose cases were recorded in an ace diagram. The perceptions were gathered and information's were communicated as mean± SD. Quantitative examination was contrasted and free example understudy's t test. Subjective investigation was contrasted and chi-square test. When utilizing these tests to think about mean among two gatherings, p-estimation of under 0.05 was taken as huge. All examinations were finished utilizing SPSS variant 16.01 factual programming Group one- Levo Bupivacaine With Normal Saline Group Two- Levo Bupivacainewithdexmedetomidine Gender Distribution
There were no statistically significant difference in the demographic profile of patients in either of the groups in terms of male to female ratio (p value-.>0.05).
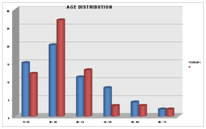
Age distribution
There were no statistically significant difference in the demographic profile of patients in either of the groups in terms of age (p value -.>0.05). Table 3: Mean Age
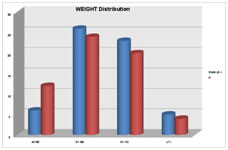
Table 4: weight (kg)
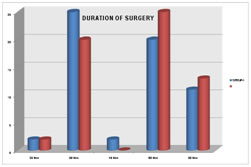
There were no statistically significant difference in the demographic profile of patients in either of the groups in terms of weight (p value -.>0.05). Table 5: Duration of surgery (in Mints)
The duration of surgery was 51.00 minutes in group one and was 55.17 minutes in group two. since p value -0.33 (0.05) statistically not significant. DISCUSSION Regular anesthesia was the most widely recognized technique for giving anesthesia to upper appendage medical procedure. With the presentation and better advantages of new and safe nearby anesthesia, territorial anesthesia has supplanted general anesthesia as a hypothetical strategy for upper appendage medical procedure. The brachial plexus square has numerous favorable circumstances over general anesthesia for upper appendage medical procedure, specifically:
Term of engine bar: The mean term of engine bar was 9.16 minutes in gathering one and 11.67 minutes in gathering two. Hence dexmedetomidine broadens the span of engine bar, which was factually critical P (<0.05), this can be contrasted and my parent study by Esmaoglu et al. Level of engine barricade: There were no measurably huge contrasts between these two gatherings with respect to the level of engine bar. The frequency of vascular cut was 6.70 in both gathering one and gathering two. There were no measurably critical contrasts among these the two gatherings. The dexmedetomidine may cause sedation without respiratory wretchedness and unfriendly impacts like hypotension, bradycardia might be seen with expanded dose. In our examination there were no measurably critical contrasts between two gatherings in regards to hemo elements yet patient had decline in pulse in gathering II contrasted with gathering I, since the p esteem (<0.05) .
Results obtained in the present study are as follows:
The study shows that:
CONCLUSIONNewer local anesthetic drugs such as levobupivacaine when combined with an adjuvant such as dexmedetomidine provide early onset of both the sensory and motor block and extend the duration of analgesia and improve the quality of the blockage with good postoperative ease of operation.
REFERENCES
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.