 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 12 Issue 3 -December 2019
A comparative study of ketamine and propofol versus fentanyl and propofol in total intravenous anaesthesia for short surgical procedures
Aditya Pradeep Reddy B1, Ballarapu Girija Kumari2*, V Ananta Kiran Kumar3
1Assistant Professor, Department of Anaesthesia, Dr Pinnamaneni Siddhardha Institute of Medical Sciences and Research Foundation, Chinoutpally, Krishna Dist, Andhra Pradesh, INDIA. 2Assistant Professor, Department of Anaesthesia, Balaji Institute of Surgery Research and Rehabilitation for Disabled, BIRRD (T)Hospital, Tirupati, Andhra Pradesh, INDIA- 517507 3Associate Professor, Department of Neurosurgery, Narayana Medical College Hospital, Chintareddy Palem, Nellore, Andhra Pradesh,INDIA. Email: drpradeep1102@gmail.com
Abstract Background: Total Intravenous Anaesthesia (TIVA) is technique of general Anesthesia using a combination of agents given solely by the Intravenous route in the absence of all inhalational agents and Nitrous oxide1.The induction of intravenous anaesthetic should be sufficient to ensure that the patient loses consciousness but not to cause undesirable side effects1. Primary aim of our study was to compare the Haemodynamic responses intra operatively in patients receiving Propofol-Ketamine and Propofol -Fentanyl in short surgical procedures and secondary outcome was to assess spontaneous eye opening and postoperative nausea and vomiting (PONV) in these patients .Materials And Methods: A prospective randomized study was done in 100 patients undergoing short surgical procedures of less than an hour duration for a period 18 months. patients were randomly selected into 2 groups of 50 each with ketamine and propofol or propofol and fentanyl. Haemodynamic response and recovery events were monitored. Results: There is significant difference in between groups in Heart Rate up to first 15 minutes, in systolic blood pressure and diastolic blood pressure. There is significant difference in spontaneous eye opening, between the groups with group PF having early recovery than PK group. There is no significant difference in duration of drowsiness, emergence reactions, nausea and vomiting when both the groups were compared. Conclusion: Propofol-Ketamine appears to be slightly better in haemodynamic stability compared to Propofol-Fentanyl. Post operative recovery is superior in Propofol-Fentanyl group than Propofol-Ketamine though the postoperative nausea and vomiting is higher in PF group which is insignificant. Key Words: Propofol, Ketamine ,Fentanyl, TIVA, Short Surgical Procedures.
INTRODUCTION Total Intravenous Anaesthesia (TIVA) is technique of general Anesthesia using a combination of agents given solely by the Intravenous route in the absence of all inhalational agents and Nitrous oxide.1 The induction of intravenous anaesthetic should be sufficient to ensure that the patient loses consciousness but not to cause undesirable side effects such as arterial hypotension and bradycardia / tachycardia1 TIVA has important role in daycare procedures requiring short duration of anaesthesia with smooth emergence from anaesthesia. Various studies have been done comparing the combination of Propofol - Fentanyl and Propofol - Ketamine and proved propofol ketamine is safe and satisfactory with less intraoperative hemodynamic disturbances and postoperative psychotic disturbances for TIVA.2,4,9,10,11 But some studies quote that propofol fentanyl has better recovery characteristics like awakening time and response to verbal commands compared to propofol ketamine combination6. There is Still controversy exists, so we intended to proceed for this study with large group of patients for a better conclusion. Primary aim of our study was to compare the Haemodynamic responses intra operatively in patients receiving Propofol-Ketamine and Propofol -Fentanyl in short surgical procedures and secondary outcome was to assess spontaneous eye opening and postoperative nausea and vomiting (PONV) in these patients.
MATERIALS AND METHODS After obtaining approval from ethics committee, a Prospective randomized study was done in 100 patients undergoing short surgical procedures of less than an hour duration for a period 18 months. All patients between 18-65 yrs of age with ASA grade 1 and 2 were enrolled in the study. Those cases with Known hypersensitivity to drugs, anticipated difficult intubation, patient refusal, pregnant and lactating mothers were excluded from study All patients were randomly selected into 2 groups of 50 each Group P K: Propofol up to 1.5mg/kg and Ketamine up to1mg/kg /body weight Group PF: Propofol upto 1.5mg/kg and Fentanyl upto 1µg/kg /body weight All patients were premedicated with Midazolam 1mg, Glycopyrrolate 0.2mg and Ranitidine 50mg I.V before shifting to operation theatre. All the standard monitors like NIBP, Pulse oximeter and ECG were connected to the patient. Propofol was given 0.5mg/kg bodyweight in all patients included in study, in PK group Ketamine was given in a dose of 0.5mg/kg bodyweight and in PF group Fentanyl was given 0.5 µg/kg body weight. Intermittent bolus doses were given when there was patient movement to surgical stimulus. Blood pressure, heart rate and saturation were recorded at the base level, at the time of induction of anaesthesia and every three minutes thereafter. Hypotension and bradycardia were recorded and treated accordingly with atropine and / Mephentaramine. Time for spontaneous eye opening after the end of surgery, response of the patient to command, postoperative nausea and vomiting, Emergence reactions like nystagmus, hallucinations and need for rescue analgesic were noted in the recovery room The following questions were asked after 30min of surgery -What is their name? -Where do they live? -What was that day and date? -does he/she has any pain? Statistical data was analysed using software package stata 13.1 Chi -square test Student t-test (paired and unpaired) was done wherever applicable. Any P value of < 0.05 was considered significant. RESULTS Table 1: Demographic data
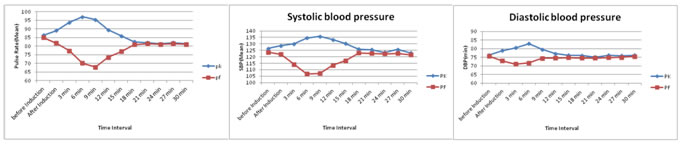
Demographic data was comparable between groups with respect to age, gender and weight. +++++ Figure 1 Figure 2 Figure 3 Figure 1: Comparison of Heart rate between the two groups; Figure 2: Comparison of systolic blood pressure between the two groups; Figure 3: Comparison of diastolic blood pressure between the two groups Figure 1, The heart rate between the two groups is statistically significant up to 15 minutes. Figure 2, There is statistically significant difference in systolic blood pressure when both groups were compared. Figure 3, There is statistically significant difference in diastolic blood pressure when both groups were compared. Table 2: Comparison of events during recovery and postoperative period
There is statistically significant difference in spontaneous eye opening, between the groups with group PF having early recovery than PK group There is no statistically significant difference in duration of drowsiness, emergence reactions, nausea and vomiting when both the groups were compared.
DISCUSSION Total intravenous anaesthesia has been a subject of interest for all the anaesthesiologists, as this is the best route to avoid operation theatre pollution. TIVA was initially attempted with a single drug e.g, (Thiopentone sodium or Propofol) but was associated with side effects and no drug was found to give complete anaesthesia. The availability of rapid and short acting sedative hypnotics, analgesics and muscle relaxants has refocused the attention on complete anaesthesia by intravenous route. The advent of continuous infusion system has made TIVA more popular and convenient. But even today we are still without any one intravenous drug that can alone provide all the requirements of anaesthesia i.e, unconsciousness, analgesia and muscle relaxation. Hence there is a need to administer several different agents to produce desired results. This in turn leads to important and significant drug interactions. In the last few decades many new sedative hypnotic drugs with improved induction, maintenance and recovery profiles have been introduced into clinical practice .Propofol is substituted phenol anaesthetic which is associated with rapid smooth induction, good maintenance and rapid recovery13,15 Ketamine is a potent analgesic, has high margin of safety. It produces no negative influence on ventilation or circulation. Its main disadvantage is emergence delirium. Fentanyl a phenyl peperidine derivative has analgesic potency 50-100 times that of morphine, but is associated with respiratory depression and postoperative nausea and vomiting. In this study comparison was done between Propofol and Ketamine versus Propofol and Fentanyl in terms of haemodynamic stability and postoperative recovery. 1) HAEMODYNAMIC PARAMETERS: a) Changes in Heart rate (HR): The mean heart rate before induction in both groups PK and PF were 86.38±8.10 and 84.98± 9.60, p value 0.432 which was statistically comparable. The mean Heart rate gradually increased in PK group up to 9 min. Heart rate gradually decreased in PF group up to 6 minutes. P value is <0.001 which is highly significant up to 18 minutes when both groups were compared. Thereafter heart rate was stable in both the groups till the end of the procedure. There was increase in heart rate after induction in PK group in study done by R. Mahajan et al7 and in present study .While there was no increase in heart rate after induction in PK group in the study by Ranju Singh et al.5 However there was decrease in heart rate in PF group after induction in above three studies. At 30min all the three studies showed heart rate comparable to that of baseline value. Heart rate does not change significantly after an induction dose of propofol. Propofol either resets or inhibits baroreceptor reflex.15 There is reduction in tachycardic response to hypotension. Heart rate may increase, decrease or may remain unchanged when anaesthesia is maintained with Propofol. Ketamine increases the heart rate by 0-59%after induction.16 The haemodynamic effects of ketamine are not dose dependent. The effect is due to increase in central sympathetic tone. Ketamine causes release of Norepinephrine which can be blocked by Barbiturates, Droperidol and Benzodiazepines. Fentanyl can cause dose dependent decrease in heart rate. Carotid sinus baroreceptor reflex of heart rate is markedly depressed by Fentanyl. These findings are also consistent with those of Shyamala Badrinath et al17 who in their study concluded that Ketamine induced tachycardia and hypotension was not evident in haemodynamic response of patients treated with Propofol-Ketamine combination. B) Changes in systolic blood pressure: In present study the systolic blood pressure of group PK and PF before induction were 126.48±5.403 and 123.52±9.199, where p value is 0.053 which is not significant. There was gradual increase in systolic blood pressure after induction in PK group up to 9min and there was fall in systolic blood pressure in PF group up to 6min.P value <0.001 is significant up to 15min when both groups were compared. Thereafter p value is not significant between two groups till the end of the procedure. Hypotension (<20% of basal blood pressure was noted in one patient in PF group which was corrected by fluid infusion and did not require any vasopressor. In study done by Ranju Singh et al5, R.Mahajan et al7 and in present study, the basal blood pressure was comparable in both groups. There was significant increase in systolic blood pressure at 3minutes after induction in PK group in study done by Ranju Singh et al5, where as in present study there was only a slight increase in systolic blood pressure. In present study there was a significant decrease in systolic blood pressure at 3 min after induction in PF group when compared to study done by Ranju Singh et al5. However at 30min systolic blood pressure was comparable in both the groups in above three studies. C) Changes in diastolic blood pressure: In present study the diastolic blood pressure of PK and PF group before induction were 76.28±6.35 and 75.6±7.70 respectively. P value 0.631. After induction there was a slight increase in diastolic blood pressure up to 6min in PK group, whereas there was a gradual decrease in diastolic blood pressure up to 6min in PF group. There was statistically significant difference in diastolic blood pressure when both the groups were compared up to 9min, P value<0.001. There was no significant difference in diastolic blood pressure in both the groups and diastolic blood pressure did not show any significant difference throughout the perioperative period. Guit JB et al2 have also reported similar trends though both groups were haemodynamically stable. The diastolic blood pressures before induction were comparable in both the groups PK and PF in studies done by Ranju Singh et al5, R.Mahajan et al7 and in present study. In the present study there was slight increase in diastolic blood pressure after induction at 3 minutes in PK group and slight decrease in diastolic blood pressure at 3 minutes after induction in PF group. However the diastolic blood pressure at 30 minutes was comparable in both PK and PF groups in all the three studies. Ketamine stimulates cardiovascular system and is associated with increase in blood pressure, cardiac index by 0-40%and 0-42% respectively. Propofol decreases cardiac index and mean arterial pressure by 40% and 10-30% respectively. Modest doses of Diazepam and Midazolam attenuate haemodynamic effects of Ketamine when given as continuous infusion. The haemodynamic stability of Propofol-Ketamine makes it suitable combination for use during outpatient anaesthesia. Sincignano et al3 studied the efficacy and tolerability of the association of Propofol-Ketamine as alternative to Propofol-Fentanyl on 40 females scheduled for short gynaecological procedures and their data suggested the association of Propofol-Ketamine reached adequate levels of anaesthesia with few and negligible effects on cardio respiratory system, thus allowing better operability and safety. The present study correlates with their study in terms of haemodynamic stability and absence of respiratory depression. Ritu Goyal et al 8 concluded that Ketamine being a cardio stimulant drug is better than Fentanyl with respect to haemodynamic stability. The incidence of apnea and respiratory depression is also less with ketamine, but Fentanyl showed faster recovery in patients where it was administered. POST OPERATIVE PARAMETERS: 1) Time for spontaneous eye opening: There was statistically significant difference with respect to spontaneous eye opening in both the groups after the end of surgery which were 6.42±1.3min and 3.64±1.2min respectively, P value <0.001 which is significant which differs with study done by R.Mahajan et al.7 Kaushik Saha et al18 in their study found that recovery time in propofol ketamine group was 11.7±7.17 minutes and in propofol-fentanyl group it was 8.7±3.28 minutes and the difference was statistically significant. Duration of drowsiness: Duration of drowsiness in both PK and PF groups were 12.72±1.61min and 7.42±1.32 min where p value (>0.01) which is not statistically significant. There was no significant difference in duration of drowsiness in both the groups done by R.Mahajan et al.7 Krishna murthy A, Sudhakar SR19 in their study concluded thatsedation using a combination of propofol 2mg/kg and ketamine 1mg/kg versus combination of propofol 2mg/kg and fentanyl 1mcg/kg for flexible bronchoscopy in patients undergoing bronchoalveolar lavage are similar in terms of haemodynamics, maintenance of oxygen saturation ,cough ,sedation levels, need for rescue doses as well as pulmonologist and patient satisfaction .The only difference being in longer duration of recovery time for propofol and ketamine group. Pandey S,Gupta s, Choudhary B et al20 concluded that both ketamine and fentanyl in propofol infusion for short surgical procedures are equally safe and effacious. Patient satisfaction is good among both groups with no significant adverse effects.Babita Ramdev, Dinesh K Sharma et al21 in their study concluded that both propofol-ketamine and propofol -fentanyl are suitable combinations as TIVA techniques as they produce rapid pleasant safe anesthesia with only a few untoward side effects and only minor haemodynamic effects. 3) Postoperative nausea and vomiting: Five patients in PK group and six patients in PF group complained of nausea and vomiting postoperatively. In the study done by Ranju Singh et al5 nausea and vomiting was higher in PK group when compared with PF group where p value was significant(0.04).Present study correlates with the study done by R.Mahajan et al7 which was comparable in both the groups in terms of PONV. Vallejo et al12 compared postoperative nausea, emesis and recovery between Propofol-Ketamine and Propofol-Fentanyl in laparoscopic tubal ligation done under general anaesthesia. The authors concluded that with Propofol-Ketamine there is no decrease in the incidence of postoperative nausea, emesis and there is no better recovery compared with Propofol-Fentanyl combination. Emergence reactions: Three patients in PK group had emergence reactions postoperatively and none of the patients in PF group. The main disadvantage of Ketamine is emergence delirium. The low incidence of emergence reactions in PK group is due to Propofol which seems to be effective in eliminating the side effects of subanaesthetic doses of Ketamine in humans.17 There was high incidence of emergence reactions in PK group in study done by R.Mahajan et al7, where as it was seen only in three patients in the present study. A variety of drugs used in the premedication or as an adjuvants during maintenance of anaesthesia have been evaluated in attempts to prevent emergence reaction after administration of ketamine. Benzodiazepines have proved more effective in prevention of this phenomenon, Midazolam being more effective than Diazepam. The low incidence of emergence reaction in PK group can be attributed to prior premedication of all the patients with Midazolam 1mg intravenously, before shifting to operation theatre. Inclusion of Thiopentone / inhaled anaesthetics may decrease the incidence of emergence delirium attributed to Ketamine. Conversly the inclusion of Atropine or Droperidol in preoperative premedication may increase the incidence of emergence delirium. A quiet recovery room and minimal interference with the patient during postoperative period can reduce the incidence of emergence phenomenon. Orientation to time, place was good in PF patients, than in PK group which is due to more drowsiness in PK group than PF group. Hallucination and dreaming were observed in three patients in PK group. Clear headedness is there in patients of Propofol -Fentanyl group.
LIMITATIONS OF THE STUDY We didn’t use variable rate continuous infusion as simple intravenous boluses is also equally effective. Modified aldrette score or Post anaesthetic discharge scoring system was not taken into consideration, instead duration of drowsiness, time for spontaneous eye opening and postoperative nausea and vomiting were taken into consideration as variables of recovery
CONCLUSION We conclude, both Propofol - Ketamine and Propofol-Fentanyl are equally safe and effective in Total intravenous anaesthesia for patients undergoing short surgical procedures. Though there is statistically significant difference in haemodynamic parameters when both groups were compared, clinically there was no significant difference. There is slight increase in systolic blood pressure in PK group after induction. In PF group, there is slight reduction in systolic blood pressure after induction. So Propofol-Ketamine appears to be slightly better in haemodynamic stability compared to Propofol-Fentanyl. Post operative recovery is superior in Propofol-Fentanyl group than Propofol-Ketamine though the postoperative nausea and vomiting is higher in PF group which is insignificant.
REFERENCES
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.