 Home
Home
|
Table of Content - Volume 14 Issue 3 - June 2020
Effect of single bolus dose of dexmedotomidine for attenuation of extubation response following general anaesthesia - A clinical study
Arathi B H1*, Sangeetha2
1Associate Professor, 2Junior Consultant, Kidwai Memorial Institute of oncology, M.H. Marigowda Road (near dairy circle) Bangalore 560029, Karnataka, INDIA. Email: arathibh@gmail.com
Abstract Background: Emergence from general anaesthesia and tracheal extubation often accompanied by Haemodynamic instability. and is of equal concern as intubation response. Tracheal extubation is accompanied by raised sympathoadrenal activity. Various options to attenuate extubation response, have been used. Alpha 2 -agonists simultaneously potentiate the effects of general anaesthetics, and attenuate sympathoadrenal responses to noxious stimuli encountered during anaesthesia, thus providing improved hemodynamic stability. Dexmedetomidine, is a highly selective alpha2 -adrenergic agonist. It has dose dependent attenuation of stress response to intubation. This study was conducted to assess the degree of attenuation of hemodynamic responses and airway reflexes to extubation by single dose dexmedetomidine infused over 10 minutes and the side effects if any. Methods: A prospective randomized controlled study, 80 patients of ASA grade I and II in the age group of 18-50 years of either sex undergoing elective surgeries under general anaesthesia were included. Group D: 40 patients received 0.5 µ/ kg body weight of dexmedetomidine diluted to 10ml in normal saline over 10 min prior to extubation Group C: Control group consisting 40 patients received 10 ml normal saline as placebo prior to extubation. Hemodynamic parameters were evaluated. Incidence of coughing, laryngospasm, bronchospasm, time to extubation and eye opening were noted. Extubation quality and sedation were rated using Extubation quality 5- point scale and Ramsay Sedation scales respectively. Results: HR, SBP, DBP and MAP were stastically lower in study group (p<0.001). Time to extubation and eye opening were prolonged in Group D (p<0.001). Incidence of coughing was significantly less in Group D when compared to control group which was significant(p<0.001). Patients were significantly sedated in study group compared to control group. Conclusion: This study demonstrates that single- dose of dexmedetomidine 0.5 µg/ kg body weight administered over 10 minutes, before tracheal extubation attenuates the airway and hemodynamic reflexes. Key Words; Extubation, haemodynamic, stress response, sedation, cough reflex.
INTRODUCTION Emergence from general anaesthesia and tracheal extubation are also often accompanied by haemodynamic instability and is of equal concern as intubation response1. Tracheal intubation and extubation are accompanied by raised sympathoadrenal activity which increase heart rate, myocardial contractility, increased systemic vascular resistance. Majority of patients tolerate these changes without any significant clinical consequences. But patients suffering from diseases like hypertension and diabetes may not tolerate these responses. Most episodes of myocardial ischemia occur during intubation and extubation. Various options to attenuate extubation response like deeper planes of anaesthesia, topical anaesthesia, use of intravenous local anaesthetics (lignocaine), calcium channel blockers (verapamil, nicardipine), opioids, sympathetic blockers (beta blockers, alpha2-agonists) etc, have been used. Alpha2 -agonists simultaneously potentiate the effects of general anaesthetics, and attenuate sympathoadrenal responses to noxious stimuli encountered during anaesthesia, thus providing improved hemodynamic, stability2. Clonidine has been studied in this aspect. Dexmedetomidine, a newer drug in this class is a highly selective alpha2 -adrenergic agonist. It has sedative, anxiolytic and analgesic actions as well. It is known to exhibit dose dependent attenuation of stress response to intubation3. This study was conducted to assess the degree of attenuation of hemodynamic responses and airway reflexes to extubation by single dose dexmedetomidine over 10 minutes and the occurrence of side effects if any.
MATERIALS AND METHODS 80 patients admitted for various surgeries done under general anaesthesia at Kidwai Memorial Institute of Oncology were included in the study. Institutional ethical committee approval was obtained. Inclusion criteria being , Patients aged between 18 to 50 years. Patients belonging to ASA physical status Grade I and Grade II. Exclusion criteria being, Patient refusal. Patients suffering from cardiac or pulmonary disease Obese patients, with difficult airway, history of sleep apnoea. patient suffering from psychiatric illness. Pre anaesthetic check up was done one day prior to the surgery. A detailed history of present and past medical illness was noted. General physical and systemic examination of the patients was done. Routine investigation and relevant specific investigations were done. Weight in kgs was recorded. Patients were advised 6 hours fasting and premedicated with Tab.Ranitidine 150mg and Tab. Alprazolam 0.5 mg on the previous day of surgery. After obtaining informed written consent, patients will be randomly divided into 2 groups. Standard general anaesthesia will be administered with:
Maintained with: Oxygen (34%) + Nitrous oxide (66%) + Isoflurane (0.4 -1%) + vecuronium as needed. Patient haemodynamic stability was maintained. depth of anaesthesia was maintained by titrating isoflurane concentration. At the beginning of skin closure, isoflurane turned off. Group I/D: Dexmedetomidine group consisting 40 patients received 0.5 µ/ kg body weight of dexmedetomidine diluted to 10ml in normal saline over 10 min prior to extubation Group II / C: Control group consisting 40 patients received 10 ml normal saline as placebo prior to extubation. Residual neuromuscular blockade was reversed using injection neostigmine 0.05 mg/ kg and injection glycopyrrolate 0.01 mg/ kg. Patients were extubated when following criteria were fulfilled. Extubation criteria to be fulfilled-
We evaluated our results by using these parameters HR, SBP, DBP, MAP, SpO2 basal, prior to drug or placebo infusion; followed by 1, 3, 5 and 10 minutes during infusion; following reversal administration; post extubation every 5 min for 30 min, thereafter every 15 min for next 1 hour. Bradycardia is defined as HR<60/min and treated with rescue dose of injection atropine 0.5mg intravenously, tachycardia being 20% increase from baseline, hypertension as either 20% increase from baseline or SBP>180mm Hg and hypotension as 20% decrease from baseline or SBP<80mm Hg. Extubation quality is rated using 5-point scale16-
Number of coughs per patient is monitored for 15 minute post extubation. Any laryngospasm, bronchospasm or desaturation noted. Time to extubation and time to eye opening, i.e. interval between cut off of nitrous oxide to extubation and eye opening respectively are recorded. Sedation evaluated using Ramsay Sedation Scale71
Statistical Methods With the power of study being 80% and confidence limits at 95% minimum sample size required to detect 30% reduction in hemodynamic parameters was 24 patients in each group. We conducted study with 40 patients in each group to make it more authentic. Descriptive and inferential statistical analysis was carried out in the present study. Results on continuous measurements were presented on Mean ±SD (Min-Max) and results on categorical measurements were presented in Number (%). Significance was assessed at 5 % level of significance. The following assumptions on data were made:
Student t test (two tailed, independent) was used to find the significance of study parameters on continuous scale between two groups (Inter group analysis) on metric parameters. Levene’s test for homogeneity of variance was performed to assess the homogeneity of variance. Chi-square/ Fisher Exact test was used to find the significance of study parameters on categorical scale between two or more groups. p value of less than 0.01 is considered statistically significant.
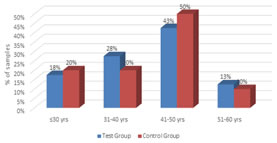
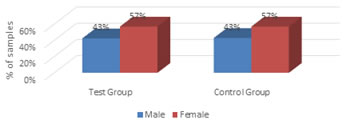
Figure 1: Age distribution of patients studied The age of the patients in both the groups are comparable and the difference in mean age between the groups is not statistically significant Figure 2: Gender distribution of patients studied The gender distribution of the patients in both the groups are comparable.
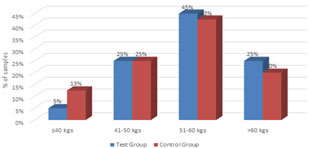
Figure 3: weight distribution of patients studied The mean weight in control group is 54.10 kgs and in study group is 56.55 kgs. Statistically insignificant difference.
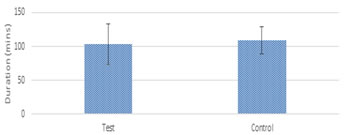
Table 1: Mean duration of surgery in two groups of patients studied
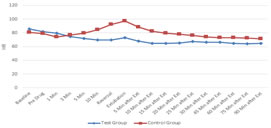
Figure 4: Mean duration of surgery in two groups of patients studied Figure 5: Comparison of HR (beats/min) in two groups of patients studied Figure 4, The mean duration of surgeries, patients underwent in both the groups is statistically comparable. Figure 5, Basal heart rate was comparable in both groups. But it was statistically and clinically lower in study group from 5th minute of drug infusion till the end of infusion; at reversal administration; extubation and post extubation 5, 10, 15, 20, 25 and 30 minutes compared to basal value. Though the above table shows statistically significant lower values at 60 and 90 minutes post extubation, they were not clinically significant.
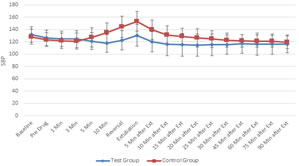
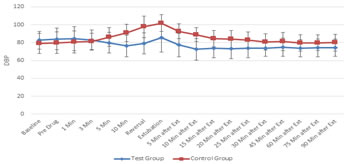
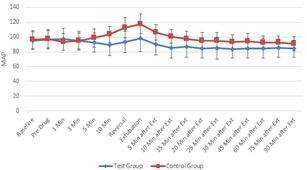
Figure 6 Figure 7 Figure 6: Comparison of systolic blood pressure (in mm of Hg) in two groups of patients studied; Figure 7: Comparison of diastolic blood pressure (in mm of Hg) in two groups of patients studied Figure 6, Both the groups were comparable with respect to basal SBP values. SBP values were statistically and clinically significantly lower in Group D at 10th minute of study drug infusion; at reversal administration; extubation and post extubation 5, 10, 15 and 20 minutes compared to basal values. SBP values in group C returned to basal levels gradually over next hour. Figure 7, Basal DBP values in both the groups were comparable. DBP values were statistically and clinically significantly lower in study group at 10th minute of dexmedetomidine infusion; at the time of reversal administration; extubation and post extubation 5, 10, 15, 20, 25 and 30 minutes compared to baseline values. DBP values at 45, 60, 75 and 90 minutes post extubation though statistically significant were not clinically significant Figure 8: Comparison of mean arterial pressure (in mm of Hg) in two groups of patients studied MAP values in both the groups were comparable at baseline. Values were statistically and clinically significantly lower in Group D compared to basal value during the period of drug infusion; at reversal; extubation and post extubation 5, 10, 15, 20, 25 and 30 minutes. MAP values post extubation 45, 60, 75 and 90 minutes were clinically not significant though statistically significant.
Table 2: Comparison of Ramsay Sedation Scale in two groups of patients studied
Patients in dexmedetomidine group were significantly sedated compared to control group at extubation and post extubation 5, 10, 15 and 30 minutes.
Table 3: Extubation quality 5- point scale (cough score) in two groups of patients studied
number of bouts of cough per patient was significantly lower in Group D when compared to Group C. Extubation quality 5- point scale was lower in study group implying smoother extubation as compared to control group.
Table 4: Comparison of Mean time to eye opening in two groups of patients studied
Time to eye opening was statistically and clinically significantly prolonged in Group D compared to Group C with P<0.001.
Table 5: Comparison of Mean time to extubation in two groups of patients studied
Time to extubation was statistically and clinically significantly prolonged in Group D compared to Group C with P<0.001.
Table 6: Comparison of complications in two groups of patients studied
10 patients in study group had hypotension which was statistically significant. This responded to intravenous fluids administration. 9 patients in dexmedetomidine group had bradycardia, but this was transient and responded to injection atropine. Laryngospasm and desaturation (SpO2< 93%) was not observed in either of the groups.
DISCUSSION Emergence from general anaesthesia and tracheal extubation is often accompanied with tachycardia and hypertension. Hartley M and Vaughan RS1 found that there is an increase of 20% in heart rate and systolic blood pressure during extubation and cause was attributed to increase plasma concentration of adrenaline. These responses may produce myocardial ischemia or infarction in susceptible patients. Alpha2 -agonists decrease the sympathetic outflow and noradrenergic activity, thereby counteracting hemodynamic fluctuations occurring at the time of extubation due to increased sympathetic stimulation.32 This study was designed to assess prospectively the degree of attenuation of hemodynamic responses and airway reflexes to extubation by administration of dexmedetomidine at the dosage of 0.5 µg/ kg body weight.. In our study both the groups were comparable with respect to age, sex, weight, ASA physical status grading and duration of surgery. HEMODYNAMIC PARAMETERS In our study we observed that HR did not show a significant rise compared to basal value from 2nd minute of drug administration, during reversal, at extubation and any period post extubation. But in control group, there was a significant rise in HR compared to basal value. The rise in HR in control group was more persistent than study group. This observation is in concurrence with the study done by Jain D et al..32 where the pulse rate in study group remained below the (baseline value) at all time intervals following extubation. Bradycardia was observed in __ 25%of patients in study group which responded to injection atropine. This is in conjunction with the observation by Aksu R et al.33 SBP, DBP and MAP values were significantly lower in study group compared to baseline values at all times from the time of dexmedetomidine infusion to post extubation 30 minutes. This is in conjunction with the study conducted by Jain D et al..32 in which study group patients received 1 µg/ kg of dexmedetomidine and they did not observe any significant change (p<0.05) in the blood pressure in dexmedetomidine group throughout the study period. On the contrary, systolic blood pressure rose significantly (p<0.05) in control group following extubation as observed in our study which we achieved with 0.5 µg/ kg of dexmedetomidine. In our study none of the patients in study group had hypertension against control group. This observation is in contradiction with the study done by Aksu R et al..33 who observed significantly increased SBP at 1 and 5 minutes after extubation. Probably this is due to infusion of dexmedetomidine over 5 minutes rather than slow infusion.
RESPIRATORY PARAMETERS Dexmedetomidine by virtue of its analgesic and sedative properties is known to blunt airway reflexes. Exutubation response was smooth extubation against patients in control group. Incidence of coughing was significantly higher in control group than when compared to study group .This is in accordance with study done by Aksu R et al.33 Guler G et al..36 they also noted the effect of dexmedetomidine on children undergoing adenotonsillectomy wherein dexmedetomidine group had significantly decreased incidence and severity of agitation and a smooth extubation without any increase in incidence of side effects. Also, the number of severe coughs per patient was significantly decreased in study drug group when compared with control group. This further supports our observation. Hence, dexmedetomidine improves extubation quality. SpO2 values were comparable in both the groups with no incidence of desaturation. Also, no bronchospasm or laryngospasm was observed in either of the groups. These observations are in concurrence with study conducted by Aksu R et al.33
COMPLICATIONS Sedation in our study was assessed using Ramsay Sedation Scale. Significant number of patients in study group were drowsy but responded to oral commands (score of 3) following extubation as against patients in control group who were co-operative and oriented (score of 2). However, those patients who were drowsy maintained SpO2with humidified oxygen administered by facemask at 4 liter/ minute which was routinely provided for all patients in PACU. This observation is in agreement with the comparative study done between dexmedetomidine and fentanyl in those undergoing rhinoplasty by Aksu R et al.33 But, in contrast to Jain D et al..32 who did not notice sedation in both the groups probably because of the difference in the anaesthetic technique employed by the authors. Sedation score was significant post extubation for __ minutes in study group compared with control group. After this period sedation scores were comparable in both the groups. EXTUBATION PARAMETERS Guler G, Akin A et al..36 in their study on emergence agitation in children undergoing adenotonsillectomy observed that time to extubation and emergence were prolonged significantly when compared to control group with p<0.05. (5.03± 2.3 vs 3.30±1.3minutes and 9.30± 2.9 vs 7.20± 2.7 minutes, respectively). This observation is in agreement with our study conducted wherein time to extubation and eye opening (i.e, interval between cut off of nitrous oxide to extubation and eye opening respectively) were significantly prolonged in dexmedetomidine group when compared to control group.
CONCLUSION In conclusion, our study demonstrates that single- dose of dexmedetomidine 0.5 µg/ kg body weight administered over 10 minutes, before tracheal extubation attenuates the airway and hemodynamic reflexes during emergence from anaesthesia providing smooth extubation without causing undue sedation. But may delay time to extubation and eye opening.
REFERENCES
Policy for Articles with Open Access
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.