 Home
Home
|
Table of Content - Volume 15 Issue 1 - July 2020
Comparison of analgesic efficacy of bupivacaine, bupivacaine and dexmedetomidine and bupivacaine and fentanyl in wound infiltration technique in perinatal surgeries: A prospective, randomized controlled study
V Haribabu1, K Gopalakrishnan2*, M Suresh Rajkumar3, V Ezhil Rajan4, R Chandrasekar5
1Associate Professor, 2Assistant Professor, 3Professor, 4,5Professor & HOD, Department of Anesthesiology, Aarupadai Veedu Medical College & Hospital, Puducherry, INDIA. Email: drkgpal73@gmail.com
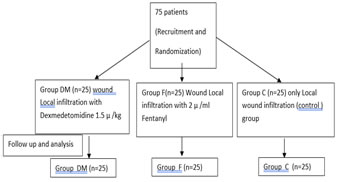
Abstract Background: Numerous methods have been proposed to alleviate pain after perianal surgeries but the role of addition of dexmedetomidine or fentanyl to bupivacaine as local infiltration in surgical wound for post-operative analgesic effect is less explored. Hence a study was conducted to compare the efficacy of wound infiltration with bupivacaine or bupivacaine with fentanyl or bupivacaine with dexmedetomidine for post operative analgesia following perianal surgeries. Methods:75 patients with ASA class of I and II scheduled for perianal surgeries were recruited for the study. The patients were randomly assigned into 3 groups namely DM, F and C. Group DM received wound infiltration with 0.5% bupivacaine 15ml which included dexmedetomidine 1.5 µg /kg, Group F received wound infiltration with 0.5% bupivacaine 15 ml which included Fentanyl 2µ/ml and Group C received wound infiltration with 0.5% bupivacaine 15 ml which included 1 ml saline. Post-operative quality of analgesia was assessed by VAS (0-10) for 24 h and rescue analgesic was administered when VAS > 4. Pain score at the time of defecation was also noted. Total dose of analgesic needed in 24 hours and side effects were noted. Results: Group DM had significantly longer duration of postoperative analgesia when compared with Group F and group C. Group F had prolonged the postoperative analgesia when compared to Group C. The pain score at first defecation was significantly lower in Group DM when compared to both Group F and Group C. None of the patients developed skin rash, respiratory depression, hypotension, hypoxemia, and there were no significant tachycardia or bradycardia. Conclusions: Wound infiltration with dexmedetomidine–bupivacaine mixture provides prolonged analgesia, and decreases the total analgesic consumption patients undergoing perianal surgeries Key Words: Analgesia, Dexmedetomidine, fentanyl, perianal surgeries, wound infiltration.
INTRODUCTION Ano-rectal disorders affect about 5% of adult population 1. Haemorrhoids, fistula-in-ano and anal fissure comprise most of them. Surgical treatment for these assures the patient a better quality of life2. Ano-rectal surgeries have conventionally been performed under general anesthesia (GA) and spinal anesthesia (SA)1. Postoperative pain is said to be most severe in anorectal surgery and thus, the choice of anesthetic methods in this procedure is crucial to reduce aches as well as postoperative complications3. Spinal anesthesia for anorectal surgery is a popular and commonly used method characterized by rapid onset and offset, easy mobilization and short hospital stay4. No matter how skillfully conducted or successful the result, almost all surgical procedures produce tissue trauma and pain. Immediate pain is very severe in anorectal surgery and difficult to control with intravenous analgesics alone3. Conventionally, nonsteroidal anti-inflammatory drugs (NSAIDs) and opiates have often been used to control pain, but their use is confined to a short period of time and is associated with frequent side effects, including gastrointestinal problems, renal dysfunction, nausea and vomiting, increased urinary retention, and reduced bowel mobility5. Also a variety of methods for reducing pain after hemorrhoidectomy and other perianal surgeries have been investigated, including pudendal nerve block, perianal infiltration of local anesthetics or botulinum toxin, and application of topical preparation such as metronidazole, glyceryl nitrate, and calcium channel blocker5. Incisional infiltration with local anesthetics has been documented to improve postoperative pain control after inguinal hernia repair or laparoscopic cholecystectomy. Infiltration with local anesthetics may also participate in providing adequate pain control after anorectal surgeries 7. Few studies have investigated the effects of addition of pharmacological agents like dexmedetomidine, fentanyl, etc to the wound infiltration in various surgeries. perianal surgeries. Few studies have studied the effects of addition of ketamine6, dexmedetomidine, etc to wound infiltration in perianal surgeries. However, there is no sufficient clinical data regarding the effects of addition of dexmedetomidine or fentanyl to the local infiltration on postoperative pain. Hence a study was conducted in Aarupadai Veedu Medical College and Hospital, Puducherry to compare the efficacy of addition of dexmedetomidine and fentanyl in prolonging the postoperative analgesia when added to local anaesthetic solution in wound infiltration technique in patients undergoing perianal surgeries.
MATERIALS AND METHODS Subsequent to receiving institutional ethical committee approval, registrations at clinical trials registry CTRI/2018/12/016807 (Registered on: 31/12/2018), and after obtaining written informed consent, American Society of Anesthesiologists (ASA) I–II patients of age 18-50 years of both gender with normal range of BMI undergoing perianal surgeries like fissure in ano, fistula in ano and haemorrhoidectomy in Aarupadai Veedu Medical College and Hospital, Puducherry from December 2018 to November 2019 were selected for the study. A prospective, placebo controlled, parallel group, double blinded, randomized clinical trial study was conducted. Randomisation was computer generated. ASA III and above, obese, underweight subjects(extremes of BMI) , pregnant women, patients with bleeding and clotting disorders, allergic to local anesthetic agents, inadequate spinal blockade supplemented by other drugs and complicated surgeries were excluded from the study. To assess pain, visual analogue scale (VAS) (0–10 cm) was utilized and instructions were given for all patients in the context of pain assessment from 0 to 10, with 0 indicating no pain and 10 indicating the worst pain imaginable during pre anaesthetic visit in the evening prior to surgery. Seventy five patients were randomly assigned into 3 groups. None of the patients received premedication. In all the three groups, surgery was done under spinal analgesia. The subarachnoid block was performed using 26G Quincke’s spinal needle in all patients in sitting position in L3–L4 space with 2.0 ml of 0.5% bupivacaine heavy. Patients were monitored with electrocardiogram, noninvasive arterial blood pressure and pulse oximetry in the operating room. Wound infiltration was performed at the end of the procedure. * Group DM received wound infiltration with 0.5% bupivacaine 15ml which included dexmedetomidine 1.5 µg /kg. * Group F received wound infiltration with 0.5% bupivacaine 15 ml which included Fentanyl 2µ/ml * Group C received wound infiltration with 0.5% bupivacaine 15 ml which included 1 ml saline.
None of the patients in either group had any complications intraoperatively. Patient was then transferred to the recovery room, and baseline vital parameters were recorded. The outcome assessor and the patient were blinded. Duration of surgery and duration of spinal blockade were recorded. Vital parameters MAP (mean arterial pressure), Pulse rate and Respiratory rate were observed every 30 min till first 2 hrs, at 6, 12, 18 and 24 hr. Hypotension was defined as a decrease in systolic arterial blood pressure >20% of baseline and was treated with intravenous (IV) 5---10 mg bolus doses of ephedrine. Bradycardia was defined as heart rate <60 beat per minute and were treated with 0.01 mg/kg bolus doses of atropine. Respiratory depression is defined as respirate rate <10 and alert was given to anaesthestiologists. Pain intensity was measured on a visual analog scale (VAS) graded from 0 (no pain) to 10 cm (the maximum pain imaginable). Pain assessment was performed at rest and movement every 2 hrs from the end of surgery till 24 hrs and at the time of the first defaecation. Any patient complaining of pain or reporting VAS >4 at any time was administered tramadol 50 mg IV slowly over 2–3 min. If pain was not relieved after 30 min and patients still complained of pain, additional doses of tramadol 50 mg IV were given, and this dose could be repeated every 30 min up to a total dose of 250 mg in 6 hours and maximum of 400 mg of tramadol over 24 h. The time of first rescue analgesic administration and total analgesic requirement in the 24 hours were noted. Hypotension was defined as a decrease in systolic arterial blood pressure >20% of baseline and was treated with intravenous (IV) 5---10 mg bolus doses of ephedrine. Bradycardia was defined as heart rate <60 beat per minute and were treated with 0.01 mg/kg bolus doses of atropine. Postoperative side effects like sedation , nausea, vomiting, headache and pruritus were recorded by the staff nurse under supervision of co investigator.
The sedation score on a 6-point Ramsey sedation scale was used.
When the patient had a sedation score of 4and above, supplement oxygen via facemask@6 L/min was administered and alert was given to the anaesthesiologist. Inj. Ondonsetron 4 mg was given slow IV for nausea and vomiting.
Statistical Analysis: Collected data were analyzed using appropriate descriptive and inferential statistics using SPSS 15.0-Software. Normally distributed interval and ratio data were analyzed using ANOVA test. Ordinal data were analyzed using Kruskal wallis test. Nominal data were analyzed using Chi square or Fischer Exact whichever was appropriate. Data was analyzed for statistical significance of p value 0.05. If the difference was found to be significant, further between groups analyses were carried out.
RESULTS No significant difference was observed between the groups with respect to gender, age, height, weight, BMI, ASA physical status and distribution of surgical diagnoses. The groups were comparable in regards to duration of surgery and duration of spinal analgesia. (Table 1).
TABLE 1: Patients characteristics and clinical data:
Ratio or interval data are expressed as mean ± SD and ASA I or II and Gender are expressed as numbers.
*DM significant to both F and C, #F significant to C
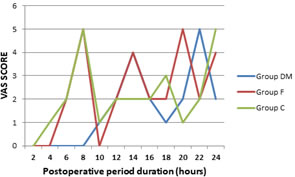
Figure 1: VAS SCORE AT REST
Median VAS score at rest and on movement of all the three groups were given in the table 2. Fig 1 shows the median value of all groups over 24 hrs. DM group had lower VAS scores than other groups till an average of 8 hours and was found to be statistically significant (p<0.01). There were no statistically significant differences in VAS scores among the groups at 10 and 12 hours intervals. But the median was lower and variation in range was narrow in Group DM. After 12 hours, the VAS scores didn’t have consistent difference.
Table 3: First analgesic request and total consumption of Tramadol
*DM significant to both F and C, #F significant to C
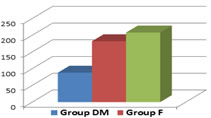
Figure 2: First Analgesic requirement (min)
The need for IV rescue analgesic for the first time was at 921.6 ± 260.89 minutes in Group DM, at 422.4 ± 61.19min in F group and at 336 ± 84.85 minutes in Group C [Table 3, Fig 2].Thus, the need for the first dose of rescue analgesia was earlier in Group C as compared to Groups DM and F and the difference was statistically significant (P < 0.05). Group DM had longer duration of postoperative analgesia when compared with Group F (p <0.05).
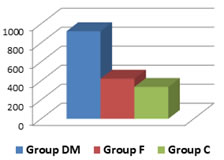
Figure 3: Total Tramadol consumption (mg)
The 24 hours analgesic requirement in Group DM was lower 88 ± 41.5 mg when compared with Group F 182 ± 24.5 mg and Group C with 208 ± 18.7 mg (Table 3, Fig 3) and the difference was statistically significant (P < 0.05). Group F had lower analgesic requirement than Group C (p <0.05).
Table 4: Pain score at First defecation
*DM significant to both F and C, #F significant to C
The Median pain score at first defecation score was lower (2) in Group DM when compared to both Group f and Group C median scores, both had 3 (p <0.05). There was no significant difference in the VAS score at first defecation between the Group F and Group C (p >0.05) (Table 4). There was no statistically significant difference between the groups in MAP (Mean Arterial Pressure), Pulse rate and Respiratory rate in all measurement intervals (p >0.05).
Table 5: Adverse event rates
None of the patients developed skin rash, respiratory depression, postoperative sedation, hypotension, hypoxemia, and there were no significant tachycardia or bradycardia. Group DM had fewer incidences of nausea vomiting than Group F and Group C, but this difference was not statistically significant (p>0.05). There was no statistical significant difference in the median sedation score among the groups (p>0.05) though Group DM had higher median sedation score (3) in the first 12 hours when compared to median sedation scores of Group F (2) and Group C (2). Among surgical procedures, fissure in ano had longer postoperative analgesia 1170 ± 103.9 minutes than Fistulectomy 700 ± 117.9 and Haemorrhoidectomy 685.3 ± 58.6 minutes (Table 6). This difference was statistically significant (p <0.05) and there was no statistically significant difference between Fistulectomy and Haemorrhoidectomy surgeries.
Table 6: DM group postoperative analgesia surgery wise distribution
*- Analgesia in Fissure patients significant from other 2 surgeries.
DISCUSSION Perianal surgeries form significant part of surgical practice. Spinal analgesia (SA) and General anesthesia (GA) techniques are the commonly administered anaesthetic techniques.for such cases. However, spinal analgesia technique seems to be simple and relatively inexpensive 8. Management of postsurgical pain is an important aspect of perioperative anaesthetic care, since acute postsurgical pain affects surgical outcomes. The post operative pain is a major cause of prolonged stay and patient dissatisfaction, necessitating the need for the anesthesiologist to provide a good postoperative analgesia that fastens patient recovery and also makes mobilization much easier 9. Wound infiltration at the end of surgery with local anaesthetic agent bupivacine for perianal surgeries is commonly followed by many and is simple to perform. To the best of our knowledge, there are only few articles on effects of addition of pharmacological agents like dexmedetomidine and fentanyl to the local solution during such postoperative wound infiltration. Dexmedetomidine, an alpha2 adrenoceptor agonist provides analgesia and sedation when administered through intravenous, epidural and intrathecal route without respiratory depression but however its synergistic action with local anesthetic agent when administered by local infiltration is not well studied10 Our current study showed significant good analgesic effect of dexmedetomidine when combined with bupivacaine in wound infiltration in perianal surgeries. Median VAS score and the range at rest and on movement of all the three groups were given in the table 2. Group DM had lower VAS scores than other groups till an average of 8 hours and was found to be statistically significant (p<0.01). Thereafter, there were no statistically significant differences in VAS scores among the groups at 10 and 12 hours intervals as Group F and Group C had already received tramadol rescue analgesia by that time. But the median was lower and variation in range was narrow in Group DM. After 12 hours, the VAS scores significance varied as each group received Tramadol injection at different point of time. Study by Abdelnaim et al..11 demonstrated that addition of dexmedetomidine with local anesthetics to wound infiltration reduces postoperative pain and also reduces the analgesic requirement which was explained by different mechanisms. The probable mechanisms are inhibition of pain conduction in C-fibers, decreasing the production of inflammatory cytokines, vasoconstrictive effect of alpha 2 agonists on vascular smooth muscle prolongs the time of analgesia, 12 Our study was similar to study by Neha Kadyan et al.12 who demonstrated that the addition of dexmedetomidine in wound infiltration with bupivacaine after abdominal hysterectomy showed reduced post-operative pain scores when compared with the control group. Another study by Vinson-Bonnet et al..7. also reported that perianal infiltration using bupivacaine with dexmedetomidine improved immediate postoperative pain control after hemorrhoidectomy, up to 6 h. Results of our study well correlated with the study of Kang et al..13 where he also observed that there was significant reduction in pain scores and fentanyl consumption in group of patients with dexmedetomidine added to ropivacaine wound infiltration than patients in group of patients with ropivacaine wound infiltration alone. Group F had lower scores than control group at 4 hours interval and it was found to be statistically significant. There was no statistically significant difference in VAS scores Between group F and group C after 4 hours. A study by Chander et al.14 reported that the mean duration of analgesia was higher in the fentanyl bupivacaine group compared to the bupivacaine alone group. This observation supports the peripheral analgesic effect of opioids. But however this combination of opioid with bupivaciane is not as effective as combination of dexmedetomidine with bupivacaine. First analgesic requirement time is longer (921.6 ± 260.89 min) in DM group than Group F group ( 422.4 ± 61.19min) and Control group (336 ± 84.85 min) (Table 3). Between Fentanyl and control groups, Fentanyl group had longer analgesia than Control group (p<0.05). A study by Selvaraj et al.15 showed that addition of dexmedetomidine to bupivacaine as local wound infiltration in port site during laparoscopic cholecystectomy prolonged the duration of analgesia, thus delayed the need for rescue analgesics in the first 8 hours of the postoperative period. Chander at al demonstrated that the requirement of analgesic was as early as 2 hours in the control group infiltrated with bupivacaine alone and the difference was as marked as 40% as compared to 3% in group where fentanyl was added to bupivacaine. In our study, total tramadol requirement in 24 hour was significantly lower in DM group (88 ± 41.5 mg) as compared to fentanyl group (182 ± 24.5 mg) and control group (208 ± 18.7 mg) (table 3). Kazemeini et al.6 in his study on the effect of local injections of bupivacaine plus ketamine, bupivacaine alone, and placebo on reducing postoperative anal fistula pain showed that the mean overall dose of opiates required by patients who was treated with wound infiltration with bupivacaine and ketamine was significantly lower than control group. Normal defecation post surgery depends on the extent of pain, duration of operation and also normal urination8. In our current study VAS score during first defaecation was lower in DM group than Fentanyl and control group (Table 4)and it was statistically significant (p<0.05). There was no significant difference in defecation score between Fentanyl group and control group (p>0.05). Kang et al.13 showed that pain score during first dafaecation was lower in ropivacaine with dexmedetomidine group than ropivacaine alone group in wound infiltration technique. Biswas et al.16 in his study observed that dexmedetomidine when added to levobupivacaine in supraclavicular block, the systolic and diastolic blood pressure values of the Dexmedetomidine Group were lower in comparison with the Control Group and that the incidence of bradycardia was higher in the Dexmedetomidine Group. Also another study by Bicer et al.17 also demonstrated a significant decrease in post-block heart rate and mean arterial pressure values in both Bupivacaine Group and Bupivacaine with Dexmedetomidine Group in comparison with the pre-block values. However, this effect lasted longer in the Bupivacaine with Dexmedetomidine Group. In our study, there were no statistically significant differences in MAP (mean arterial pressure), heart rate and respiratory rate among the three groups. The study by Aksu et al.18, addition of dexmedetomidine to the bupivacaine for TAP block and the study by Abdelnaim et al...(11), addition of dexmedetomidine to the bupivacaine wound infiltration for herniorrhaphy surgeries showed that there was no statistically significant difference in the incidence of nausea and vomiting. Similar to them, in our current study, there was no significant difference in the incidence of nausea vomiting among the groups (p<0.05) (Table 5). Bielka et al.19 in his study on dexmedetomidine infusion as an analgesic adjuvant during laparoscopic сholecystectomy showed there was no inter-group difference in the incidence of postoperative sedation. However other studies by Xiao et al.20 and Manne et al.21 showed a higher incidence of sedation in the dexmedetomidine group. In our study, there was no statistically significant difference in sedation score between groups (p>0.05) though DM group had higher median sedation scores than those of Fentanyl and control group in first 12 hours. None of them needed oxygen supplementation in their postoperative period. Within the DM group, Fissure in ano patients had a longer postoperative analgesia 1170 ± 103.9 min than other Haemorrhoidectomy patients 685.3 ± 58.6 and fistula in ano patients 700 ± 117.9 and the difference was statistically significant (p<0.01) (Table: 6)
CONCLUSION Dexmedetomidine added to bupivacaine in wound infiltration at the end of surgery in perianal surgeries significantly reduces postoperative pain, 24 hours analgesic consumption and the pain score during first defecation. Dexmedetomidine is superior additive than Fentanyl.
REFERENCES
Policy for Articles with Open Access
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.