 Home
Home
|
Table of Content - Volume 15 Issue 1 - July 2020
Comparative effects of intravenous diclofenac versus intramuscular diclofenac on post-operative surgical pain management
Richa V Patel1, Neha G Vasava2*, Mayur B Kachchhi3
1Assistant Professor, 2Senior Resident, Department. Of Anaesthesiology, GMERS Medical College, Valsad, INDIA. 3Critical Care Physician And Intensivist, Unity Trauma Center And ICU, INDIA. Email: drricha2087@gmail.com , dr.nehavasava@gmail.com , mayurkachchhi@gmail.com
Abstract Background: Postoperative pain management is a vital factor contributing towards speedy recovery of the patient in the perioperative period without significant morbidity. The present study was designed to study the efficacy, duration of analgesia and adverse effects of intramuscular and intravascular diclofenac in laproscopic surgery with changes in heart rate, blood pressure, respiratory rate and pain score during post-operative period. Methods: This case control study was conducted during 2016 to 2017 at Civil Hospital, Ahmedabad, Gujarat. Patients belonging to 18 to 50 years age group with ASA grade I and II of either sex undergoing laproscopic surgery and fit for surgery under general anaesthesia were included. They were randomly allocated to two groups. Group A was given 75 mg IM diclofenac and Group B was given 75 mg IV diclofenac 30 mins before extubation. Post-operative vitals and pain scores were monitored. All raw data were entered into an excel spread sheet and analysed by SPSS 16.0 and GRAPHPAD software. Results: Mean age of patients in Group A and B were 37.96 ± 9.28 and 36.16 ± 8.84 years respectively. Group A had 18 male patients and 7 female patients while group B had 16 males and 9 females. Duration of Action was 7.24 ± 1.31 hours and 6.96 ± 0.84 hours in group A and group B respectively. There was no significant difference in post-operative pulse rate, systolic BP, diastolic BP, respiratory rate and VAS pain score between the two groups. Conclusion: We concluded that both Intramuscular as well as Intravenous Diclofenac sodium are almost equally effective in relieving post-operative pain. Diclofenac is one of the safe and effective modality for post-operative pain relief without any significant side effects. Keywords: ASA, Diclofenac, post-operative pain, VAS.
INTRODUCTION Postoperative pain control is a major concern for doctors and the patients.1 Pain in post-operative period is an emotional and mental trauma with unpleasant sensory experience. Excessive leads to adverse effects like hypertension, tachycardia, increased myocardial work, psychological distress, immobility, respiratory discomfort and delayed recovery. Effective post-operative pain control is an essential component to reduce mortality and morbidity following surgery.2 Postoperative pain not only affects the patients operative outcome, well-being, and satisfaction from medical care, but also directly affects the development of tachycardia, hyperventilation, decreases in alveolar ventilation, transition to chronic pain, poor wound healing, and insomnia, which in turn may impact the operative outcome.3 It is also the basic duty of an anaesthesiologist to provide pain relief in both intra operative as well as immediate post-operative period. Numbers of pharmacological and non-pharmacological approaches are being used for relief of post-operative pain and investigations are still under way to find out the best method or pharmacological agent for post-operative analgesia.4 The use of opioid drugs for the pain control during and after surgery is a common procedure in anesthesia. However, the use of these medications is associated with side effects such as nausea, vomiting, sedation, respiratory depression, pruritus, urinary retention.5 Non-steroidal anti-inflammatory drugs are usually effective for mild to moderate pain control. The effectiveness of these drugs has been identified as opioids adjuvant for moderate to severe pain.6 Diclofenac is an effective and well tolerated NSAID recommend for treatment of acute painful and inflammatory conditions. It is a non-selective COX inhibitor and aryl acetic acid derivative. It is most commonly widely used NSAID, employed for managing post-operative pain, due to its short duration.7 With this background, the present study was designed to study the efficacy, duration of analgesia and adverse effects of intramuscular and intravascular diclofenac in laparoscopic surgery with changes in heart rate, blood pressure, respiratory rate and pain score during post-operative period.
MATERIALS AND METHODS Present study was conducted during 2016 to 2017 at Civil Hospital, Ahmedabad, Gujarat. Ethical committee approval was sought before commencing the study. Patients belonging to 18 to 50 years age group with ASA grade I and II of either sex undergoing laproscopic surgery and fit for surgery under general anaesthesia were included in the present study. Patients with ASA grade III and IV, cardiovascular, Hepatic and Renal dysfunction, with severe hemodynamic instability like severe anaemia, hypotension, patients with history of bleeding and coagulation disorders, acid peptic disease, severe asthma, hypersensitivity reaction and opioid abuse were included. All patients were examined on the day before surgery and explained about the anaesthetic technique and peri-operative course. Informed and written consent of patient was taken before including them in the study. Pre-anesthetic checkup for each patient was include-any significant present/past medical history, history of any previous surgery with significant anaesthetic complication and history of present or past medication and history of drug allergy. Assessment of Airway and vital parameters like BP, Pulse, Respiratory rate, Body Weight, Height were done. Routine investigations like: CBC, RFT, LFT, FBS, ECG, Chest X ray and other investigations if patients physical condition warrants any. Patients were advised to remain NBM for at least 6 hrs. before surgery. In operation theatre ECG, NIBP, SpO2 were applied and 18 G intravenous cannula was inserted into a suitable vein and secured. All patients were pre oxygenated with 100% O2 for 3-5 minutes via bain circuit and Pre-medicated with Inj. Glycopylorate (4 mcg / kg) I.V. , Inj. Fentanyl (1-2 mcg/kg) I.V. , Inj. Emset ( 0.1-0.2 mg/kg ) I.V. Induction was done by Inj. Propofol (2 mg /kg) I.V. and Inj. Succinyl choline (1-2 mg/kg) I.V. Patient was Intubated with appropriate sized portex, cuffed, ET tube and Maintained with O2, N2O and Sevoflurane. Inj. Vecuronium I.V. (0.1 mg/kg loading and 0.02 mg/kg for maintenance) was given as a muscle relaxant. Ventilation was adjusted to maintain ETCO2 35-40 mm Hg and intra abdominal pressure will be maintained between 12-14 mm of Hg. 30 mins before end of the laparoscopic procedure these patients were randomly allocated to Group A or Group B each group having 25 patients.
Patients were reversed with Inj. Glycopyrolate (8mcg/kg) IV and Inj. Neostigmine (0.05mg/kg) IV. And extubation was done after proper oral and endotracheal suctioning. After surgery, patients were transferred to the postoperative ward. HR, BP, and pain scores were recorded immediately after surgery and at 30 min, 4, 12 and 24 hour after surgery. Pain scores were evaluated using a 0–10 VAS (0 - no pain to 10 - worst pain imaginable).8 Severity of pain was determined by using the visual analogue scale. It uses a straight line with extremities of pain intensity on either end. The line is typically 10 cm long with one end defined as “no pain” and the other end being “excruciating unbearable pain”. To assist in describing the intensity of pain, words can be placed along the scale (e.g., mild, moderate, or severe). Such descriptors can help to orient the patient for the degree of pain; this particular variation of the VAS has been known as a graphic rating scale. Inj. Tramadol was used as rescue analgesia when VAS score>4. Statistical analysis All raw data were entered into an excel spread sheet and analysed by SPSS 16.0 and GRAPHPAD software. Categorical variables (egg demographic parameters like sex, ASA physical status) were analysed using Pearson’s Chi square test. Normally distributed numerical variables such as VAS score, consumption of post-operative systemic analgesics, and antiemetic between two groups were analysed using unpaired t-test. Data was expressed as mean values ± standard deviation (SD). P value <0.05 was interpreted as clinically significant and P value >0.05 considered as non-significant.
OBSERVATIONS AND RESULTS In this study 50 patients were taken and were divided in two groups of 25 patients each. Group A patients received I/M Diclofenac 75mg while group B received I/V Diclofenac 75 mg. Rescue analgesics were given as per the individual requirement of the patients. As per the table 1, mean Age, Sex distribution and ASA status of the patient in all groups were nearly same without any significant differences.Table 1: Age, Sex Distribution and ASA Status of Patient
Table 2: Duration of Surgery
There was no significant difference in duration of surgery as it was almost similar in both groups and duration of action of drug in both groups. (Table 2)
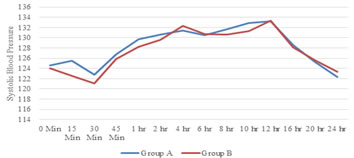
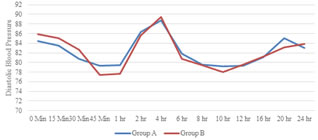
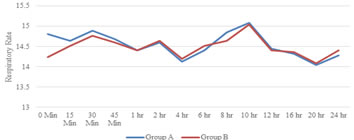
Figure 2: Monitoring of systolic blood pressure over the period of 24 hours Figure 3: Monitoring of diastolic blood pressure over the period of 24 hours Figure 4: Monitoring of respiratory rate over the period of 24 hours
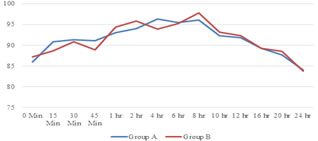
There was no significant difference in pulse rate of patients in both the groups. P value was not significant. (Figure 1) There was no significant difference in systolic blood pressure in both groups. P value was not significant. (Figure 2) There was no significant difference in diastolic blood pressure in both groups. P value was not significant. (Figure 3)
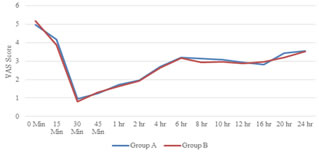
Figure 5: Monitoring of Visual Analog Score over the period of 24 hours There was no significant difference in VAS in both groups. P value was not significant. (Figure 5)Table 3: Rescue Analgesia Requirement
Table no. 3 shows that there was no significant difference between time of rescue analgesic and number of rescue analgesia in both the groups. There was no difference in incidence of complication between both the groups. (Table 4) Table 4: Complications
DISCUSSION Recently non-steroidal anti-inflammatory drug diclofenac sodium has been studied by many authors and has been found effective for post-operative pain relief. Diclofenac Sodium is established drug used for post- operative analgesia since many years. Narcotic analgesic have been used as a drug of choice for post-operative pain by different routes like intravenously, intrathecally, in infusion pump as per the requirement of the patient (PCA) but because of many side effects other group of drugs are used. Different drugs in use are morphine, tramadol and fentanyl. Nowadays better drugs with minimal adverse effects and more profound analgesic effect have been evaluated. NSAIDS leads to dyspepsia, gastric erosion and haemorrhage. Pain after laparoscopic surgery has three different components: Incisional pain (somatic pain), Visceral pain (deep intra-abdominal pain) and Shoulder pain (referred to visceral pain). Inadequately treated pain can result in various complications like atelectasis/ pneumonitis/ hypoxemia, deep vein thrombosis, delayed recovery of bowel function, myocardial ischemia and infarction, urinary retention and residual psychological trauma.9 That is why pain relief in perioperative period is very important. Selection of Patient: Aim to provide postoperative pain and study efficacy of intravenous vs intramuscular diclofenacin laparoscopic surgery, we studied 50 patients of ASA 1/ 2, and divide them into two equal group. Induction was done with inj. thiopentone sodium (5-7 mg/Kg/iv) and inj. succinylcholine (1.5-2 mg/Kg/iv). Patients were intubated with proper size cuffed endotracheal tube then maintained on O2, N2O and sevoflurane (1-2%) and inj. Vecuronium loading and maintenance dose. Group A was given 75 mg IM diclofenac and Group B was given 75 mg IV diclofenac 30 mins before extubation. Perioperative vitals, RR and post-operative VAS score and side effect noted and rescue analgesic (Inj. Tramadol 2mg/kg IV) was given to patients if they complained of pain or if VAS score was greater than 4 postoperatively for 24 hours. In our study Group A and Group B patients showed that there is decrease in pulse rate and blood pressure once the patient was relieved of pain. As the analgesic action of the drug vains off pulse rate and blood pressure start rising. Goel et al..10 in their comparative study for preemptive analgesia with intramuscular and intravenousDiclofenac sodium in patients undergoing various surgical procedures, found that heart rate was almost equal to base line value in both the groups. Similarly in our study heart rate were comparable in both the group. Debashish Paul et al..11 compared diclofenac as postoperative analgesic in two different groups in 68 patients. They assessed SBP, DBP and MAP in both the groups and observed that there is no significant variation in both the groups in different intervals. Postoperative rapid shallow breathing is a feature of inadequate pain relief. In our study, there was no significant difference found in respiratory rate between both the groups. So, it’s suggestive that both the drugs have not any deleterious effect on respiratory pattern. In our study majority of patients didn't complain of any pain at least upto 6 hour after administration of drug. After then few of them (5 patients of group A and 6 patients of group B) needed rescue analgesia. Wininger et al..12 reported the results of a randomised double-blind placebo-controlled clinical trial evaluating the analgesic efficacy of repeated doses of two dosing regimens of IV diclofenac (75mg) versus placebo in 244 patients with moderate to severe postoperative pain after abdominal laparoscopic surgery. Patients in both IV diclofenac dosing groups experienced statistically significantly greater pain reliefover 24 hours compared with placebo (1000 mg q6h, p < 0.007; 650 mg q4h, p < 0.019). MI. Tawalbeh13 concluded that Diclofenac has good analgesic effect which decreases pain on swallowing and as a result of that patients started taking orally earlier in adenoid surgery. Similar study was done by Debashish Paul et al..11 who compare diclofenac as post-operative analgesic in two different groups in 68 patients found no significant difference in VAS Score. Manjunath K.R et al..14 studied analgesic activity of IM diclofenacand IV Diclofenac as preemptive analgesic in patients who underwent laparoscopic surgeries, which showed significant reduction in postoperative pain. They found that number of rescue analgesics in control group during the postoperative period was found to be comparatively almost similar. When the total numbers of rescue analgesics amounts for 24 hour were compared of both group patients there was no significant difference in doses of analgesia underwent laparoscopic surgeries. In our study we found that time of rescue analgesia is almost similar in group A patient (6.44 ± 0.44) compared to group B patients (6.5 ± 0.43). And total number of rescue analgesia is almost comparable in group A (2.68 ± 0.47) patient compared to group B (2.72 ± 0.45) patients. Debashish Paul et al..11 also found that patients who were administered diclofenac had shown better outcome with less requirement of rescue analgesia. In our study, fewer cases of nausea (8% cases in each group) and vomiting (4% cases in each group) in both group patients noted which was managed by medication easily. Debashish Paul et al..11 have found that patients in the both diclofenac group had more incidences of complications like nausea and vomiting. Malhotra HB et al..15 studied effect in different surgeries and as per his study 11% of patients in diclofenac group had episodes of nausea and vomiting. Christian C. Apfel et al..16 did study of side effect of diclofenac compared to IV opioids, and concluded that when IV diclofenac was given prophylactically, the reduction of nausea correlated with the reduction of pain, but not with opioids. So we can conclude that diclofenac is better choice as far as side effect is concerned compared to opioids Because diclofenac spare the side effects of opioids like respiratory depression, constipation and urinary retention.
CONCLUSION We concluded that both Intramuscular as well as Intravenous Diclofenac sodium are almost equally effective in relieving post-operative pain. Diclofenac is one of the safe and effective modality for post-operative pain relief without any significant side effects.
REFERENCES
Policy for Articles with Open Access
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.