 Home
Home
|
Table of Content - Volume 15 Issue 3 - September 2020
Evaluation of supraclavicular brachial plexus block using a nerve stimulator versus ultrasound guidance
Anupriya1, Abhimanyu Tarkase2*, Shailendra D Chauhan3, Sudhir Deshmukh4
{1Junior Resident III, 2Associate Professor, 3Professor, Department of Anesthesiology} {4Professor, Department of Surgery} SRTR Medical College Ambajogai , Beed 431517 Maharashtra, INDIA. Email: yadavanupriya1@gmail.com
Abstract Background: Peripheral nerve blocks can be performed by several methods. The present study was undertaken to compare the peripheral nerve stimulator (PNS) and ultrasound guided (USG) supraclavicular brachial plexus block in terms of time taken for block, onset and duration of sensory and motor blockade, success rate and incidence of complications. Methods: Total 100 patients aged between 18-60 years, posted for upper limb surgeries were randomized into two groups of fifty each. Group 1 (PNS) received total dose 30 ml (20 ml bupivacaine 0.5% +10 ml 2% lignocaine with adrenaline (1:2lakh) in a dose of bupivacaine 0.5% - 2mg/kg and lignocaine with adrenaline (1:2 lakh) 5-7mg/kg). Group 2 (USG) received Inj. bupivacaine 0.5% reducing the dose required to 25% i.e total dose 25ml (15ml bupivacaine 0.5%+ 10ml 2% lignocaine adrenaline (1: 2 lakh ) according to body weight and dose of bupivacaine 0.5% 2mg/kg and lignocaine with adrenaline (1:2 lakh) maximum 5-7mg/kg). Results: The greater success rate found in ultrasound guided (92%) than PNS guided (82%) supraclavicular block, which was not statistically significant. The mean time taken for the procedure was 7.52 min in group1 whereas in group 2 it was 8.52 min. Onset of sensory and motor block was early in group 2 compared to group 1. Duration of analgesia was similar in both the groups. Incidence of complications like vessel puncture was seen more in PNS technique as compared to ultrasound group. Conclusion: Ultrasound guided technique is safe and effective means of performing peripheral nerve blockade with a comparable success rate. Key Words: Supraclavicular, Peripheral, Stimulator, Ultrasound, Sensory blockade, Motor blockade, Bupivacaine, Lignocaine, Adrenaline
INTRODUCTION Peripheral nerve blocks are cost effective anaesthetic techniques used to provide good quality anaesthesia and analgesia while avoiding airway instrumentation and hemodynamic consequences of general anaesthesia. Patient satisfaction, a growing demand for cost effective anaesthesia and a favourable postoperative recovery profile have resulted in increased popularity for regional techniques. Brachial plexus block is an easy and relatively safe procedure for upper limb surgeries.1 Various approaches like supraclavicular, interscalene, infraclavicular and axillary have been used for blocking brachial plexus block are associated with rapid onset and reliable anaesthesia2. Among these approaches, supraclavicular block is one of the most commonly practiced approach for brachial plexus block since it provides consistent and predictable anaesthesia of the entire upper extremity. The first supraclavicular brachial plexus block was performed by Kulenkampff in 19123. However, the classical approach using paraesthesia technique is a blind technique and may be associated with higher failure rate and injury to the nerves and surrounding structures4. To avoid some of these problems use of peripheral nerve stimulator was started in 1962 by Greenblatt and Denson which allowed better localization of the nerve/plexus5. Since the last few decades, nerve stimulator was considered the gold standard for performing the peripheral nerve blocks. However this technique may not be foolproof with persistent risk of injury to surrounding structures, especially vascular structures, nerves6 and pleura leading to pneumothorax7. Grange et al.... in 1978 8 reported the use of Doppler USG in performing supraclavicular block by identifying subclavian vessels. The use of USG helps in identifying the brachial plexus and to guide the needle thereby minimizing the risk of injury to the nearby structures. Hence, the present study was undertaken to compare the above two techniques for performing supraclavicular block with respect to efficiency and complication rate.
MATERIALS AND METHODS This prospective randomized observational study was conducted in 100 patients of either sex, ASA Grade I-III, aged between 18-60 years undergoing elective upper limb surgery lasting more than thirty minutes at Tertiary Care Hospital during a period from December 2017 to October 2019. After obtaining Institutional Ethical Committee approval and written informed consent from all the patients the study was started. Patients not willing for study, having age <18 years and >60 years, patients with significant coagulopathy, peripheral neuropathy, history of relevant drug allergy, asthma, COPD, diabetes, hypertension and patients having difficult intubation were excluded from the study. All the patients underwent thorough pre-anaesthesia evaluation on the day prior to the surgery. All systems were examined including airway and the surface anatomy where the block was going to be given and the procedure to be carried out was explained. They were informed about development of paresthesia. Patients were reassured to alleviate their anxieties. All the patients were kept nil per oral as per the fasting guidelines. All of them received Tab. Diazepam 10mg and Tab. Ranitidine 150mg night before the surgery. All relevant investigations included Hb%, BT, CT, Urea, Serum creatinine, blood sugar, blood grouping and cross matching, urine albumin, sugar and microscopy, ECG and Chest x-ray PA view depending on the age were done and associated comorbidities were noted. Intravenous line was started with 20G intravenous cannula on the contralateral upper limb under aseptic techniques. All the patients were premedicated with ranitidine 1mg/kg i.v, ondansetron 0.08mg/kg i.v and midazolam0.02mg/kg before the procedure. Patients were divided into two groups of 50 patients in each group. Group 1 (Peripheral nerve stimulator) received supraclavicular brachial plexus block using PNS total dose 30ml (20ml bupivacaine 0.5%+ 10 ml 2% lignocaine adrenaline (1: 2 lakh ) according to body weight. Group 2 (Ultrasound guided) received USG supraclavicular brachial plexus block using total dose 25ml (15 ml bupivacaine 0.5% +10 ml 2% lignocaine with adrenaline (1:2lakh). Pulse oximeter, non-invasive blood pressure were monitor on the opposite side upper limb, respiratory rate, electrocardiography. Ultrasound machine and probe were prepared for the procedure under all aseptic precautions. PNS machine with all connections in working conditions. Patient was made to lie supine with the head turn opposite to the site of intended block and arm adducted and pulled down gently. A small pillow or folded sheet was placed below the shoulder to make the field more prominent. A point 1cm above the midpoint of clavicle and pulsations of subclavian artery were done. Parts were prepared for the block to be performed with betadine solution. Anatomical landmarks were identified and skin wheal was raised using lignocaine 2% 2-3ml solution. In USG group, block was performed after real time visualization of the vessels, nerve and bone. In the plane approach using 10ml syringe containing local anaesthetic was injected and the drug distribution was noted. In PNS group, block was performed after adequate and required motor response at current 0.2 to 0.5 mA using 10 ml syringe containing local anaesthetic solution and disappearance of motor response was noted. The time taken for the procedure, onset and duration of sensory and motor blockade was noted. Intra-operatively, hemodynamics was monitored at regular intervals. Following completion of surgery, patients were monitored to assess the quality and duration of post-operative analgesia. Thus patients were asked to classify analgesia as no pain, mild pain, moderate pain or severe pain every hour for the first 6 hours and then again at 8 and 10 hours and 12 hours up to 24 hours. At the time of each subsequent assessment, patients were observed and/ or questioned about any subjective and/or objective side effects (sedation, nausea, vomiting or respiratory depression, neurological injury). Data was collected every 5mins for the first 15 mins, next at 30min and for every 30 mins till the end of surgery and at least for 24 hours postoperatively. Assessment of complete recovery of both sensory and motor blockade was done for at least 24 hours postoperatively. Results were statistically analyzed using Chi-square test and Unpaired t test. A P<0.05 was considered significant.OBSERVATIONS AND RESULTS The demographic profile of the patients was comparable and found no significant difference between two groups as shown in table 1. Both groups had predominantly males accounting for nearly 2/3 of the total study population in each group.
Table 1: Demographic profile of the patients
ORIF plate was the most common surgery performed in both the groups and other upper limb surgeries performed under supraclavicular block are depicted in figure 1.
Figure 1: Upper limb surgeries performed under Supraclavicular block
Time taken for the block performed by ultrasound was little longer than the peripheral nerve stimulator technique, which was not significant. Onset of sensory and motor block was early in group 2 (USG) as compared to group 1(PNS) and it was statistically significant. Duration of sensory and motor blockade as well as duration of analgesia were similar in both the groups and found no significant difference as shown in table 2. Table 2: Characteristics of supraclavicular brachial plexus blocks
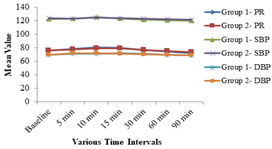
Haemodynamic parameters such as pulse rate (PR), systolic blood pressure (SBP) and diastolic blood pressure (DBP) at various time intervals were comparable between two groups, (P>0.05) as shown in figure 2. Figure 2: Comparison of haemodynamic parameters
In group 1, the block was successful in 41 (82%) cases while remaining 9 (18%) patients required general anaesthesia. In group 2, total effective block was observed in 46 (92%) patients and remaining 4 (8%) required general anaesthesia. This was statistically non-significant as the P value was 0.137 (P>0.05). Incidence of complications like nausea and vomiting, vessel puncture was seen more in peripheral nerve stimulator technique as compared to ultrasound group, (Figure 3). Figure 3: Comparison of Intra-operative complications between two groups
DISCUSSION Supraclavicular approach has been routine used in our institution for upper limb surgeries and it has been proven to be safe technique as well. We used less volume of drug in group 2 which was performed via ultrasound as USG helps in better visualization and directing the needle near to brachial plexus compared to group 1 which was PNS guided. The demographic profile of the patients was comparable between two groups which is comparable with the previous studies 9, 10. There was no other co-morbidity observed in the study. Time taken for the block performed by ultrasound was little longer than the peripheral nerve stimulator technique as the administration of the block was done by Residents posted in the orthopaedic operation theatre, it means that expertise is required to administer and use ultrasound machine. Although few other studies have proved that US-guided technique was performed faster than PNS-guided technique 9, 11. Authors of some studies have observed longer time taken for the block performance found in group USG can be explained as the less experience and skills in using the ultrasound. Morros et al...12 suggest that the use of ultrasound in regional anaesthesia requires the acquisition of new knowledge and skills not only by anaesthesiologist in training but also by anaesthesiologist experienced in nerve stimulation guided peripheral nerve blocks, showing at least 15 ultrasound-guided axillary blocks are required before good results can be expected with the new procedure. The mean onset time of sensory and motor block was significantly shorter in USG group as compared to the PNS group; this is similar to the study done by Marhofer et al.13 and Ratnawat et al.14. Duration of sensory blockade in PNS group was 422.2 ± 137.9 minutes and in USG group it was 447.4 ± 95.99 minutes (p value=0.29) so there was almost similar postoperative analgesia duration in both the groups. Thus, the duration of sensory and motor blockade was similar in both the groups and this is comparable with the previous studies9, 15. Various criteria have been used by different authors to determine the success rate of a block. A block is considered successful by most of the authors when analgesia is present in all areas subjected to surgical intervention. This definition is sufficient from a clinical point of view, but implies a falsely high success rate and makes comparison of different block techniques difficult. Therefore to standardize the criteria of success, we consider our block successful when analgesia was present over all areas supplied by four major nerves, incomplete nerve block was defined as the absence of sensory block in at least one neuronal distribution and/or the need for another anaesthetic (GA) technique to allow surgery 16. In existing study, most of the patients had successful brachial plexus block and hence satisfactory surgical anaesthesia. A successful brachial plexus block depends not only on the technique used, but also on the experience of the anaesthetist, patient's body habitus, amount and type of drug injected, the level of motivation of the patient, and the definition of a successful block11. Failure of block defined as inadequate or patchy analgesia even after 30mins of the drug administration. Depending on the effectiveness of the block the patient was being administered sedative and analgesic in the form of IV inj. Midazolam(0.02mg/kg) and Inj.fentanyl(2ug/kg). In the case of complete failure general anaesthesia was administered. In present study, out of 50 patients in group 1, 9(18%) blocks were failed and needed supplementation in the form of general anaesthesia while in group 2, 4 (8%) blocks were failed and needed supplementation in the form of general anaesthesia which was not statistically significant. These findings are correlated well with other studies 9, 17, 18. Complications like vessel puncture formation occurred in the PNS group 14%; whereas in ultrasound group it as 4%, because ultrasound provides direct visualization of vessel around the plexus and also needle path, this complication was less in USG group. We can also take the help of Doppler to visualize the vessels. The study did not found any other major complications like nerve injury or pneumothorax in both of the group. These findings are in accordance with the study done by Yuan et al.19 and Singh et al.20. In current study, the ultrasound guidance allowed fewer needle punctures and fewer vascular punctures compared to PNS guided method due to visualization of vascular structures it gave us an advantage to prevent vessel injuries. One of the most important advantages of using US for brachial plexus block is the direct visualization of the needle tip in relation to the cervical pleura, thus minimizing the chances of an accidental pleural puncture. Also, it can determine the size, depth, and exact location of the plexus and its neighboring structures. A preblock anatomical estimation can be done, which can help avoid complications and improve success rates as well as provide confidence to the anesthesia provider21. Also due to the correct needle placement and visualization of the spread of drug, smaller than usual amount and volume of drug can be used to achieve a satisfactory and dense blockade.
Limitation of the Study There was no blinding in the data collection which was a possible source of bias in the present study. The moderate experience of the specialist might have contributed to more procedural times but this need not possibly affect the outcome with respect to major study parameters.
CONCLUSION From the results of present study, it can be concluded that ultrasound guided technique is safe and effective means of performing peripheral nerve blockade with a comparable success rate and less intra-operative complications.
REFERENCES
Policy for Articles with Open Access
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||


 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.