 Home
Home
|
Table of Content - Volume 15 Issue 3 - September 2020
A study of effect and side effects of thermal radiofrequency nerve ablation of genicular nerves for the management of chronic osteoarthritis of knee joint
Tsering Yougyal1*, Vijay Kumar Sauhta2, Jasa Ram Thakur3, Girish Sharma4, Shweta Mahajan5
1Department of Health & Family Welfare Himachal Pradesh Government, Operation Theatre Incharge Civil Hospital Joginder Nagar, Distt Mandi, Himachal Pradesh, INDIA. 2Operation Theatre Incharge Civil Hospital Theog Shimla Himachal Pradesh, INDIA. 3Department Of Health & Family Welfare HP Government, Operation Theatre Incharge Zonal Hospital Mandi Himachal Pradesh, INDIA. 4Professor, Department of Anaesthesia, Dr Y. S. Parmar Govt medical college, Nahan, District Sirmour, Himachal Pradesh, INDIA. 5Associate Professor, Department of Anaesthesia, Indra Gandhi Medical college, Shimla. Himachal Pradesh, INDIA. Email: yougyal1001@gmail.com., d.sauhta@gmail.com, jassathakur821@gmail.com
Abstract Background: Pain is the most prominent symptom of osteoarthritis of knee joint. It is most common reason to seek help in patients. Present study was conducted to record the level of satisfaction after thermal radiofrequency ablation. Aim and objective: To record the level of satisfaction after thermal Radio frequency ablation in patients of osteoarthritis of knee joint. Methodology: Present study was a randomized double blinded controlled prospective study carried out in 50 patients with osteoarthritis of knee joint. Patients were studied under 2 groups. Group I was control group where No thermal or Pulsed radiofrequency was given. In Group II thermal radiofrequency was given. Patients in both the groups were compared for level of satisfaction. Results: The difference in mean Satisfaction level Post- procedure was found to be statistically insignificant (Mean ± S.D: 1.48 ± 0.510 vs 1.44 ± 0.507) in Groups I and II respectively (p-value=0.782). There was statistically highly significant difference in the Satisfaction level between group I and group II at 1st week till the consecutive follow up till 12th weeks after the procedure (p-value <0.001). Key Word: thermal radiofrequency nerve ablation.
INTRODUCTION Along with the increase in age, there is an exponential increase in the associated risk factor of obesity, due to progressive sedentary behaviour, changes in lifestyle patterns, diet routine, and work environment conditions among the adult population. Currently 80% of persons affected by OA knee joint already report having some movement limitation, and 20% report not being able to perform major activities of daily living. 1 OA can be seen as a degenerative, chronic, and often progressive joint disease. Despite the development of newer imaging technique, the radiograph remains the most accessible tool in the evaluation of the OA joint. Obesity has a strong correlation to the development of OA and weight loss programs have significant impacts on the development and progression of OA. One study found that the probability of developing OA of the knee was decreased by 50%, in a linear fashion, with a 10 pound weight loss over 10 years. 2 Diet and exercise regimens are even more beneficial; several trials demonstrated that the combination of diet and exercise improved quality of life, knee pain, and mobility among patients with knee OA. Physical therapy, which aims to strengthen supporting muscle groups and improve flexibility, is a mainstay therapy for OA. Patients report pain relief, decreased stiffness, and improved mobility through physical therapy. Furthermore, physical therapy may delay the need for surgical intervention. Genicular nerves have been selected for 2 reasons. First, the genicular nerves are the main innervating articular branches for the knee joint, and second, as these nerves are adjacent to the periosteum connecting the bone, they can be located using bony landmarks under x-ray imaging. More specifically, the postulated mechanism of action for clinical benefit of Thermal RFA involves the heat generation resulting in thermo coagulation and localized neuronal tissue destruction. These lesions have been shown to demonstrate the characteristics of scar formation, including an acute inflammatory response, cell necrosis and fibrosis with collagen fiber deposition, occurring over 3 weeks following the procedure. It has been shown that the basal lamina of Schwann cells may be preserved after RFA (Radiofrequency Ablation), which would allow nerve regeneration.3—5 The ablative heat is provided via flow of electrical current, generating a well-delineated lesion. Additionally, RFA produces a local electrical field, which is thought to promote neuromodulation by inhibition of the excitatory C-fibers. 5,6 Various studies have been done to see the effectiveness of RFA in the treatment of pain related to osteoarthritis of knee joint. Present study was conducted to record the level of satisfaction after thermal Radio frequency ablation in patients of osteoarthritis of knee joint. Aim and objective: To record the level of satisfaction after thermal Radio frequency ablation in patients of osteoarthritis of knee joint.
MATERIAL AND METHODS After approval from institutional ethics committee and written informed consent, 50 adult patients of ASA Grade 1 and 2, aged between 40 - 70 years, and diagnosed clinically with osteoarthritis of knee joint during the period from July 2016 to Jan 2017 were recruited in the study. The study was conducted in randomized double blinded controlled prospective manner. Inclusion criteria: 1. Patients between Stage 1 and Stage 3 radiological changes, according to the Kellgren-Lawrence classification 13 2. Patients with Age from 40 to 70 years.3. Patients with Pain localised to knee joint with no referred pain. 4. Patients without visible gross structural deformity of the knee joint. 5. Patients within ASA Grade I and II. 6. Patients on conservative treatment such as physical therapy, analgesic drugs including NSAIDs or opioids, for at least six months Exclusion criteria: 1. Patients refusal for the intervention. 2. Patients at Stage 4 radiologically, according to the Kellgren Lawrence classification. 3. Patients with Age less than 40 and more than 70 years. 4. Patients with visible gross deformity of the knee joint. 5. Patients of ASA Grade III or more. 6. Existence of general contraindications against application of invasive intervention 7. Psychiatric disorders. The enrolled patients after fulfilling all the inclusion and exclusion criteria were randomly allocated to two equal groups (n=25 in each group) using computer generated random number list. The random number was kept in envelope under custody and was opened in intervention room at the time of procedure, and the patients were allocated to the group according to the random number. Post procedure observation and follow up were made by independent anesthetist not associated with the block giving team. GROUP I Control group. (n = 25): Under all possible aseptic conditions, radiofrequency cannula was placed extra articularly around the knee joint under C-Arm guidance targeting the superomedial, superolateral and inferomedial genicular nerves. After satisfactory placement, the stylet in the cannula was removed and RF probe (Cosman RFK, Cosman medical inc, USA) was placed through the cannula and motor (2 hz and 0.5 V) and sensory (50 Hz and 0.2 V) stimulation was done. After localizing the above mentioned Genicular nerve, 1 ml of 1% lidocaine was injected at each needle site and waited for two minutes. No thermal or Pulsed radiofrequency was given. Patient shifted to the recovery room and observed for any side effects or complications for up to one hour. GROUP II Radiofrequency group. (n = 25) :Under all possible aseptic conditions, radiofrequency cannula was placed extra articularly around the knee joint under C-Arm guidance targeting the superomedial, superolateral and inferomedial genicular nerves. After satisfactory placement, the stylet in the cannula was removed and RF probe (Cosman RFK, Cosman medical inc, USA) was placed through the cannula and motor (2 hz and 0.5 V) and sensory (50 Hz and 0.2 V) stimulation was done. After localizing the above mentioned Genicular nerve, 1 ml of 1% lidocaine was injected at each needle site and waited for two minutes. Then radiofrequency was given with target temperature at 70 degree Celsius for three cycles each of 1.5 minutes duration. Following the procedure, patients were transferred to the recovery room and observed for one hour for any possible side effects or complications and was discharged after one hour. Post procedure observation and follow up were made by independent anaesthetist not associated with the block giving team. During the 1st, 4th, 8th and 12th week, they were asked to attend the pain clinic date on the specified days (Wednesday/Saturday) or were contacted on phone and inquired about Level of satisfaction. It was noted as 1- Excellent 2- good 3- Not satisfied. All the data were then collected and systematically recorded, tabulated and statistically analysed using student t-tests and the results thus obtained were presented in the light of statistical and clinical significance.
RESULTS Total number of patients enrolled during study period was 50, with 25 patients each in group I (control group) and group II (study group). In this study, both the groups were comparable in demographic variables like age (table II), weight (table III) and sex (table IV). There were more number of female patients in both the group with total number of 31 out of total 50 patients (i.e. 62%) and 19 out of 50 patients (i.e. 38%) were males. Both the group were comparable and statistically insignificant (p values >0.05). General physical examination and investigation of all the patients were within normal limits. Out of the 50 patients recruited for the study, 15 patients (30 %) were ASA I and 35 patients (70%) were ASA II. The baseline heart rate (Table V) was 83.56 ± 5.760 bpm and 83.32 ± 5.956 bpm in group I and group II respectively with p value = 0.885. The baseline mean arterial pressure was 98.76± 8.084 mmHg and 97.92 ± 9.151 mmHg in group I and group II respectively with p value = 0.732. The baseline mean Spo2 was 94.44 ± 2.162 % and 94.72 ± 2.264 mmHg in group I and group II respectively with p value = 0.657. All these baseline parameters were comparable in both the groups. The mean heart rate initially and during the procedure was statistically insignificant and comparable amongst the two groups. (table 1) The mean arterial pressure initially and during the procedure was statistically insignificant and comparable amongst the two groups. (fig 1) The mean respiratory rate initially and during the procedure was statistically insignificant and comparable amongst the two groups. (fig 2) The mean oxygen saturation (Spo2) initially and during the procedure was statistically insignificant and comparable amongst the two groups. (table 2) In group I, immediately during the post procedure period, out of 25 patients, 13 patients gave excellent review while 12 patients said it was good showing that they were satisfied with the procedure but by the first week of follow up, all the patients in the group I starting experiencing pain of the knee joint and the whole 25 patients in group I was not satisfied from 1st to 12th weeks of follow up. While in group II, initially in the post procedure period, out of 25 patients in the group, 14 patients gave excellent review and 11 patients said it was good, which is similar to the immediate post procedure reviews of group I patients too. At 1st week follow up, out of 25 patients, 6 patients gave excellent review and 18 patients said it was good while one patient was not satisfied. On further follow up at 4th week, 2 patients gave excellent review, 22 said it was good and same one patient was not satisfied. At 8th week follow up, 1 patient gave excellent review, 23 said it was good and one patient was not satisfied. On the final follow up at 12th week, out of 25 patients of group II, all 24 patients said that the effect of intervention done 12 weeks back was good, while one patient, who was not satisfied from 1st week of follow up consistently said that she was not satisfied. The difference in mean Satisfaction level initially (i.e. Post- procedure) was found to be statistically insignificant (Mean ± S.D: 1.48 ± 0.510 vs 1.44 ± 0.507) in Groups I and II respectively (p-value=0.782) and was comparable. However, there was statistically highly significant difference in the Satisfaction level between group I and group II at 1st week till the consecutive follow up till 12th weeks after the procedure (p-value <0.001). (Table 3). Table 1: Comparison of mean heart rate between both groups
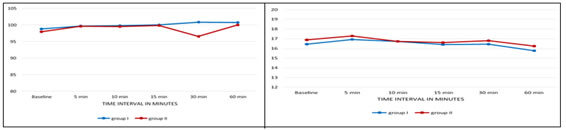
Figure 1: Comparison of Mean Arterial Pressure (MAP) in Figure 2: Comparison of mean respiratory rate between two groups both groups Table 2: Comparison of Oxygen Saturation (SPO2) in two groups
Table 3: Comparison of satisfaction level between the two groups
DISCUSSION In the current study, we asked the patient’s overall experience, whether they are satisfied with the intervention with the grading of Level of satisfaction as : 1- Excellent, 2- good and 3- Not satisfied. The mean satisfaction level post procedure immediately, at 1st week, 4th week, 8th week and at 12th week with group I was 1.48 ± 0.510, 2.96± 0.200, 3.00± 0.00, 2.96 ± 0.200 and 3.00 ± 0.000 respectively and with group II was 1.44 ± 0.507, 1.80 ± 0.500, 1.96 ± 0.351, 2.00 ± 0.289 and 2.04± 0.200. In the immediate post procedure period, the difference in satisfaction level was statistically insignificant (p >0.05). At one week of follow up and onwards upto 12th week of follow up, the difference in the satisfaction level between two groups were statistically highly significant (p < 0.001) as more patients were satisfied in group II. In group I, immediately in the post procedure period, out of 25 patients, 13 patients gave excellent review while 12 patients said it was good showing that they were satisfied with the procedure but by the first week of follow up, all the patients in the group I starting experiencing pain of the knee joint and the whole 25 patients in group I was not satisfied from 1st to 12th weeks of follow up. While in group II, initially in the post procedure period, out of 25 patients in the group, 14 patients gave excellent review and 11 patients said it was good, which is similar to the immediate post procedure reviews of group I patients too. At 1st week follow up, out of 25 patients, 6 patients gave excellent review and 18 patients said it was good while one patient was not satisfied. On further follow up at 4th week, 2 patients gave excellent review, 22 said it was good and same one patient was not satisfied. At 8th week follow up, 1 patient gave excellent review, 23 said it was good and one patient was not satisfied. On the final follow up at 12th week, out of 25 patients of group II, all 24 patients said that the effect of intervention done 12 weeks back was good, while one patient, who was not satisfied from 1st week of follow up consistently said that she was not satisfied. The results were only comparable immediately after the post procedure period which can be explained by the use of local lidocaine after localisation of the genicular nerve. The patients in the group II was highly satisfied with the results ranging from good to excellent whereas most of the patients in the group I was not satisfied with the procedure from the first week of follow up. It was comparable with the similar studies done by Choi et al.. where the RF group patient satisfaction was better than the control group satisfaction at 4 and 12 weeks. 7 Similarly in the study of by Ferdinand Iannaccone et al.., out of all 31 procedures, 74% provided the response that they were satisfied and would recommend RFA of genicular nerves to a family member or loved one. 8 In the current study, no complications such as infection, haemorrhage, thermal injury, or sensory or motor loss in the procedure area developed in any of the 50 patients. There are similar outcomes in many previous studies, namely Choi et al.. several participants experienced temporary periosteum touch pain from the RF canula during the procedure, the pain was tolerable and required no medication. Otherwise, no participant reported a post-procedure adverse event during the follow up period, and there were no withdrawals from the study owing to an adverse event.7 This is further supported by the study of Pakize KIRDEMİR et al.., where out of total 49 patients recruited in the study, no complications such as infection, haemorrhage, thermal injury, or sensory or motor loss in the procedure area developed in any patient. 9
CONCLUSION Thermal radiofrequency ablation provides an excellent satisfaction in pain relief in patients with osteoarthritis of knee joint.
REFERENCES
Policy for Articles with Open Access
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.