 Home
Home
|
Table of Content - Volume 17 Issue 1 - January 2021
A comparison between prophylactic IV ephedrine hydrochloride and crystalloid preloading for prevention of post-spinal hypotension
Palakben Parikh1, Jayshree Thakkar2*
1Assistant Professor, Department of Anaesthesiology, NHL Municipal Medical College, Ahmedabad, Gujrat, INDIA. 2Professor, Department of Anaesthesiology, Gujarat Cancer and Research Institute, Ahmedabad, Gujrat, INDIA. Email: dr.palak.parikh@gmail.com
Abstract Background: To evaluate and compare the effectiveness of prophylactic IV Ephedrine and prophylactic crystalloid preloading for prevention of postspinal hypotension and their complication. Methodology: This study was conducted in 60 adult patients with ASA grade I and II who were undergoing for lower abdominal and lower limb surgeries. Patients were randomly divided into two groups. Each group had 30 patients. GROUP I received prophylactic injection Ephedrine 3 mg IV stat as soon as SAB given then Ephedrine infusion at 1mg/min for 15 minutes started. GROUP II received Crystalloid preloading at 20 ml/kg over 20 min before SAB given. HR, SBP, DBP, SPO2% and ECG changes were noted at every 2 minute for a period of 20 minute and then every 10 minute till the end of surgery. Patients were observed for any immediate or late complications. Observations and Results: Age, weight, gender and duration of surgeries are comparable in both groups.HR is higher in group I but statistically insignificant. Hypotension is recorded in 10% patients in group I while 23.33% patients in group II. There is significant fall in SBP and DBP in preloading group (p<0.05). Dose of rescue ephedrine is higher (7.28±1.6 mg) in preloading group than (3±0 mg) in ephedrine group. Conclusion: Prophylactic IV Ephedrine as minimal initial bolus followed by IV infusion is a simple, easy, economical, effective and reliable method to prevent hypotension, intraoperative nausea, vomiting and shivering. This is comparable with Crystalloid preloading group with minimal side effects like tachycardia Key- Words: Ephedrine infusion, preloading, hypotension, spinal anaesthesia
INTRODUCTION Spinal anaesthesia was introduced into clinical practice by August Bier in 1898. Spinal anaesthesia is considered as gold standard anaesthesia due to its advantages like avoidance of intubation, earlier return of GI function, lower incidence of post operative thromboembolic events etc. Hypotension is dangerous outcome occasionally found in spinal anaethesia due to sympathetic block. Its prevention or timely intervention is key management in spinal anaesthesia. Prophylactic leg elevation, preloading with crystalloids and colloids, lateral uterine displacement in obstrectic patients and vasopressors are various measures to reduce severity of hypotension. Ephedrine is the most commonly used vasopressor to treat spinal induced hypotension1,2. We performed prospective randomised controlled study in lower abdominal and lower limb surgeries to compare the efficacy of prophylactic IV Ephedrine hydrochloride and preloading for prevention of postspinal hypotension.
AIMS AND OBJECTIVES: To evaluate and compare the effectiveness of prophylactic IV Ephedrine and prophylactic crystalloid preloading for prevention of postspinal hypotension and their complication.
MATERIAL AND METHODS This study was conducted at Gujarat cancer and research institute, BJ Medical College, Ahmedabad in 2010-2013. Ethical approval was taken from INSTITUTIONAL RESEARCH COMMITTEE (IRC). Patients undergoing elective lower abdominal and lower limb surgeries were included in the study. Patients with systemic diseases like diabetes, hypertension, bleeding disorders, heart diseases and anaemia were excluded. Pre-operative evaluation and written informed consent were taken. Preoperative sedation was given at night as tablet lorazepam 1 mg stat orally and in morning as Tab Diazepam 5 mg stat orally. Patients were randomly divided into two groups; each group included 30 patients as follows: GROUP I: Prophylactic Ephedrine 3 mg IV stat as soon as SAB given and Ephedrine infusion at 1mg/min for 15 minutes started. GROUP II: Crystalloid preloading at 20 ml/kg over 20 min before SAB given. Intravenous cannula N. 18 G was inserted and baseline HR, SBP, DBP and SPO2 measured in operating room. Lumber puncture was done in left lateral position by using 23 G spinal needle in L3-4 space with all aseptic and antiseptic precautions. After free flow of CSF, Inj Bupivacaine (hyperbaric) 4 ml of 0.5% and Inj Fentanyl 25 mcg injected in subarachnoid space. Supine position with 10 degree trendelenberg position was given. Small pillow was placed under shoulder. Onset of sensory analgesia was determined by pinprick method. Final dermatomal level of analgesia was noted after 20 minutes of subarachnoid block. HR, SBP, DBP, SPO2% and ECG changes were noted at every 2 min interval for a period of 20 min and then ever 10 min until the end of surgery. Patients were observed for any immediate or late complications. STATASTICAL ANALYSIS: Data calculation and p value calculation is done by unpaired t-test using online software from http://www.graphpad.com/quickcalcs/ttest1/?Format=SD.
OBSERVATION AND RESULTS Total 60 adult Patients belonging to ASA I and II were selected for the study. Each group received 30 patients. Table I: (Age, weight and gender)
Age, weight and gender characteristics are comparable in both groups [statistically non-significant (P>0.05)].
Table II: (Type of Surgery)
Table III: (Level of block)
This table shows that onset of analgesia were comparable in both groups and statistically nonsignificant (P>0.05).
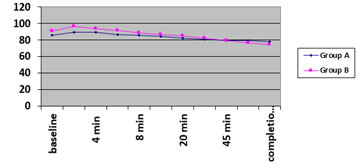
Table IV: [changes in heart rate(bpm)]
(*p<0.05) This table shows that HR significantly increases from baseline at 2 minutes in both groups.
Graph1: Changes in heart rate in both groups
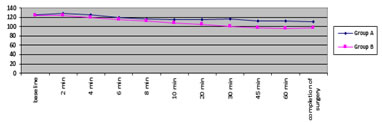
Table V: [(changes in systolic blood pressure (mm hg)]
*p<0.05 This table shows in group II there was significant fall in SBP after 10 minutes till completion of surgery.
Graph 2: changes in systolic blood pressure in both groups
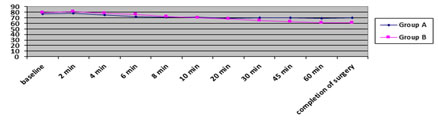
Table VI: [changes in diastolic blood pressure(mm hg)]
(*p<0.05) This table shows that in group II, there was significant fall in DBP after 20 minutes (p<0.0001) till completion of surgery
Graph 3: changes in diastolic blood pressure in both groups
Table VII: (incidence of hypotension)
This table shows that incidence of hypotension which was more in group II (23.33%) as compared to group I (6.66%).
Table VIII: (dose and time for rescue ephedrine)
(*p<0.05) This table shows that need for rescue ephedrine was more in group II than group I and time for need of rescue ephedrine was much earlier in group II than group I.
Table IX: (incidence of complications)
This table shows that complication like nausea, vomiting, shivering and bradycardia were more seen in group II.
DISSCUSION Spinal anaesthesia induced hypotension is treated physiologically by improving the venous return which increase preload and restore the cardiac output. Position of head down or leg elevation (10-15") or leg wrapping with elastocrep bandage does not abolish the incidence of hypotension3,4 Crystalloids on the other hand are required in great volumes(>15ml/kg) to decrease the incidence of hypotension5, These large volumes have detrimental effects like: Increased central venous pressure6 , blood dilution leading to decrease in oxygen carrying capacity7, release of atrial natriuretic peptide initiating diuresis, thereby attenuating the effect of volume load on blood pressure8. Due to the above consideration it seems appropriate that prophylactic administration of a pharmacologic agent is more effective than prehydration for prevention of hypotension9,10,11. Among the Vasopressors a mixed adrenergic agonist such as Ephedrine more ideally corrects the non cardiac circulatory sequelae of spinal anaesthesia than does either a pure α-or β-adrenergic agonist12 Studies of prophylactic bolus or infusions of IV Ephedrine have proved their efficacy in preventing the episodes of hypotension without unwanted side effects13,14,15 So we conducted this study to determine the safety and efficacy of prophylactic IV Ephedrine bolus 3 mg with infusion at 1mg/min for next 15 min and its comparison with crystalloid preloading in reducing the incidence of hypotension, nausea, vomiting and shivering after SAB. In our study selected 60 adult patients of ASA grade I and II were comparable in age , sex ratio(M: F) and undergoing elective lower abdominal and lower limb surgeries. Onset of sensory analgesia (mins) was comparable, (8.84±2.32) in group I and (8.53±1.96) in group II(p>0.05). In our study sensory analgesia up to T6 level was attained in 60 %of patients in group I and 63.33% in group II, T8 level in 23.33% in group I and 20% in group II. In our study, we used preloading of Ringer Lactate at 20 ml/kg over 20 min before SAB which is comparable to SONIA OUERGHI et al.16 In our study we used total dose of prophylactic dose of Ephedrine was total 18 mg. It was first given as a 3 mg bolus as soon as SAB given and then 1mg/min for next 15 minutes. The total dose of ephedrine we have used is comparable to LIONEL SIMON et al.17 They studied 10, 15 and 20-mg prophylactic boluses of IV Ephedrine for prevention of hypotension in caesarean section. KANG, Y. G et al18 studied Prophylactic intravenous Ephedrine infusion(0.01 % solution, beginning with approximately 5mg/min) versus prophylactic bolus (20 mg) during spinal anaesthesia for caesarean section. In patients given the infusion, SBP did not change significantly from the base line SBP following spinal anaesthesia (p>0.1) and reactive hypertension did not occur. The results suggested that prophylactic ephedrine infusion is safe and desirable than bolus under spinal anaesthesia which is comparable to ephedrine infusion in our study. In our study we defined hypotension as fall in SBP>=30% from baseline. Incidence of hypotension was more in group II (23.33%) than in group I (6.66%). In group I nonsignificant (p>0.05) fall in SBP and DBP after 20 minutes while in group II there was fall in SBP and DBP after 20 minutes were highly significant(p<0.001). In group I only 2 patients while in group II 7 patients developed hypotension after 20 minutes required more than one bolus of Inj. Ephedrine 3 mg till SBP increases 70% of baseline. Total mean dose of rescue ephedrine (mg) used in group I was 3±0 mg while in group II, it was 7.28±1.6mg (p<0.05). The first rescue ephedrine time in the ephedrine group was significantly longer (47.5±3.5 min vs. 21.5±4.6 min) than that of the preloading group (P<0.0002). Our results are comparable with NOOR M.GAJRAJ et al.19 who studied comparison of efficacy of an Ephedrine infusion (5 mg/min for the first 2 min and then 1 mg/min for the next 18 min ) with crystalloid (15 ml/kg) administration for reducing the incidence of hypotension during spinal anaesthesia in patients scheduled for PPTL. The incidence of hypotension was higher (55%) in the crystalloid group than (22%) in the infusion group (p<0.05). Fall in SBP after 20 min was more in preloading group than ephedrine group(P<0.01), which is comparable to our study. The crystalloid group received a boluses of rescue ephedrine mean (mg) of 1.4±1.9 and the infusion group received a mean (mg) of 0.4±0.8 boluses (p<0.05) which was comparable to our study. The first rescue ephedrine time in the ephedrine group was significantly longer (14.9±7.1 mins vs. 7.9±5.4 mins) than that of the control group (P<0.05) in Iclal et al.20 study which is comparable to our study. Hypertension developed in 6 (28.6%) patients in Iclal et al. study. High doses of prophylactic IV ephedrine are associated with significant side effects like reactive hypertention. In our study, 5(16.66%) patients developed reactive hypertension due to ephedrine in group 1. In our study initially rise in HR in both groups after 2 min (p<0.05) can be due to effect of Inj. Glycopyrrolate. In preloading group, 4 (13.33%) patients developed bradycardia which was treated by inj. Glycopyrrolate. In group I, 10 patients developed tachycardia (pulse>=20% from baseline) which was treated by selected beta blocker Inj. Esmolol 20 mg IV stat. Our results were comparable to Iclal et al.20 They studied that 0.5 mg/kg intravenous ephedrine over 60 sec. causes tachycardia in ephedrine group which was 52.4%(11 patients and(6 patients)28.6% in control group which was statistically insignificant(p>0.05). No patients developed bradycardia in ephedrine group and three (14.3%) in control group (p<0.05) As Ephedrine increases MAP and presumably improve medullary blood flow. Incidence of nausea alone or with vomiting during spinal anaesthesia was 16% in preloading Group and 2% in Group ephedrine in our study which is statistically significant (p<0.05). This is comparable to ROTHENBERG DM et al.21 study who concluded that ephedrine is an effective antiemetic agent. Youn Yi Jo et al.22 studied to determine the effect of ephedrine on intraoperative hypothermia of patients undergoing spine surgery. They concluded that an intraoperative infusion of ephedrine minimized the decrease the core temperature which is comparable to our study. We had (3.33%) patient developed shivering in ephedrine group while five (16.66%) patients in preloading group.
CONCLUSION Prophylactic IV Ephedrine as minimal initial bolus followed by IV infusion is a simple, easy, economical, effective and reliable method to prevent hypotension, intraoperative nausea, vomiting and shivering. This is comparable with Crystalloid preloading group with minimal side effects like tachycardia.
REFERENCES
Policy for Articles with Open Access: Authors who publish with MedPulse International Journal of Anesthesiology (Print ISSN:2579-0900) (Online ISSN: 2636-4654) agree to the following terms: Authors retain copyright and grant the journal right of first publication with the work simultaneously licensed under a Creative Commons Attribution License that allows others to share the work with an acknowledgement of the work's authorship and initial publication in this journal. Authors are permitted and encouraged to post links to their work online (e.g., in institutional repositories or on their website) prior to and during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work.
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.