 Home
Home
|
Table of Content - Volume 18 Issue 2 - May 2021
Prospective randomized study to determine the suitable prophylactic dose of intramuscular injection ephedrine to prevent hypotension following subarachnoid block
Shobha Vatkar1*, Shilpa Gurav2
1Assistant Professor, 2Professor and HOD, Department of Anesthesiology, MIMER Medical College. Talegaon(D), Pune, INDIA. Email: shobhavatkar@gmail.com
Abstract Background: Spinal anaesthesia is a commonly practiced mode of regional anaesthesia for adult patients undergoing elective operations for lower abdomen and lower extremities region. As hypotension develops rapidly, optimal SAP (Systolic Arterial Pressure) control is mandatory. The primary objective of this study is to prevent hypotension after spinal anaesthesia by using intramuscular vasopressor; injection ephedrine. The secondary objective is to evaluate the effectiveness of two different intramuscular fixed doses 15mg [E15] and 30mg [E30] of injection ephedrine given 10 minutes prior to spinal anaesthesia to find out the suitable dose in maintaining hemodynamic stability after subarachnoid block. Material and Methods: Sixty adult patients scheduled for elective operation under spinal anaesthesia (SA) were investigated for two groups. Systolic arterial pressure (SAP) Mean arterial pressure (MAP) and pulse rate were noted, before spinal anaesthesia and after spinal anaesthesia at various intervals till 60 minutes. Onset of Hypotension, hemodynamic variables, and first rescue dose of ephedrine, total ephedrine consumption, adverse drug interactions and other complications were recorded. Results: Degree and incidence of hypotension (SAP and MAP) were more in [E15] group than [E30] group .SAP was maintained with [E30] group without significant percentage change .It remained optimal at 40 minutes time after subarachnoid block. Occasional rise in the HR was seen with [E30] group. Total rescue dose of ephedrine consumption were more in [E15] group compared to [E30] group. Intermittent ventricular extrasystoles were noted in 30mg group which were insignificant. Conclusions: Prophylactic intramuscular injection ephedrine, in the dose of 15mg and 30mg, given 10 minutes prior to subarachnoid block, do avoid hypotension following spinal anaesthesia. Among these 30mg of injection ephedrine achieved sufficient hemodynamic stability during the procedure in comparison to 15mg dose. So 30mg prophylactic IM dose of injection ephedrine given 10 minutes prior may be an effective fixed dose to prevent hypotension following spinal anaesthesia in adult elective cases. Keywords: Ephedrine, Hypotension, Blood pressure, Spinal anaesthesia, Intramuscular
INTRODUCTION Spinal anaesthesia is a commonly practiced mode of regional anaesthesia for adult patients undergoing elective operations for lower abdomen and lower extremities region. However it is found that around 25-75% patients who undergo operations under spinal anaesthesia do develop hypotension during the procedure.1 Hypotension following spinal anaesthesia mainly occurs due to sympathetic blockade leading to peripheral vasodilatation and venous pooling of blood. As a result, there is decreased venous return and cardiac output leading to hypotension. Development of hypotension has various clinical manifestations such as nausea, vomiting which often interfere during surgery2 Techniques currently in use for prevention of hypotension include: preloading with crystalloid or colloid optimizing patient's position(Tredelenberg position) use of leg bindings, compression stockings administration of vasopressors, with varying degree of success.3 InjectionEphedrine, Phenylephrine and Mephenteramine sulphate are the most widely used vasopressors in current practice. Ephedrine is sympathomimetics which stimulates alpha and beta adrenergic receptors, and also releases nor adrenaline from its storage site. Ephedrine was introduced as vasopressor into anaesthetic practice in 19274 Its modern synthetic compound remains a drug of choice to treat hypotension induced by spinal or epidural anaesthesia.5 The main effects of therapeutic doses of ephedrine are cardiac stimulation and elevation of systolic and usually diastolic blood pressure through an increase in cardiac output and peripheral vasoconstriction9 Several published randomised controlled and prospective studies found the efficacy of ephedrine for the treatment and prophylaxis of hypotension with spinal anaesthesia administered through intravenous (IV) route. Patients were administered bolus dose in the range of 5 mg to 10mg with larger doses observed to provide greater efficacy. Most of the studies reported dose titration using rescue IV ephedrine as a single bolus dose of around 2.5mg to 10mg, incremented as required when the SAP or MAP fell. On an average dose required to be 10mg to 30mg. Reactive hypertension is seen when the dose exceeds 30mg intravenous (IV). The efficacy varied between the studies which may have been attributed to the administration of timing of injection, the route and the dose of ephedrine used. Overall the literature suggest the use of ephedrine in the treatment of hypotension secondary to spinal anaesthesia administered through an IV bolus dose and with additional incremental rescue boluses as required to the effective dose. There is potential regarding harmful Hypertension and tachycardia with ephedrine in high IV dose administration.5,6,7,8 It has been used by many routes i.e. Intravenous, Intravenous plus IM and only Intramuscular with varying time interval by different studies in the past. The purpose of this study is to find out suitable IM dose of injection Ephedrine to prevent hypotension for adult elective cases done under subarachnoid block. The recommended dose for Intravenous (IV)route of injection Ephedrine is 10-25mg; while the dose for IM or SC rout is 25-50mg (range 10-50mg9. The duration of presser and cardiac response of ephedrine remains for 1 hour. There were different intramuscular and intravenous dose recommendations by different studies earlier. All of them in past assessed the effects of prophylactic administration of intramuscular (IM) ephedrine for prevention of hypotension following spinal anaesthesia. In our proposed study, we have studied the two different doses 15mg and 30mg of IM ephedrine, given 10 minutes prior to subarachnoid block to find out the suitable dose for preventing hypotension following spinal anaesthesia in adults for elective cases, without any side effects.
MATERIAL AND METHODS After obtaining approval from Ethical committee of MIMER Medical College, Talegaon Dabhade, Pune (IEC/MIMER/2019/647), the current prospective and comparative study was conducted from October 2019 to February 2020. The sample size was calculated with power of 80% with an alpha error of 0.05 and confidence interval 95% and required 60 adult patients for recruitment. Inclusion criteria: Sixty adult patients classified by American Society of anaesthesiologist as ASA-PS grade I and II involving both the sexes, undergoing elective operations under spinal anaesthesia, in the age group of 18 to 65 were enrolled in this study and were divided in two groups (E15 and E30 group) Exclusion criteria: Patients with Spinal anaesthesia level above T6, ASA(American Society of Anesthesiologist) physical status III and above, Patients on anticoagulant / Respiratory, CNS and Psychiatric disorders, Paediatric patients, pregnant females, and Patients who refused regional anaesthesia and patients having bleeding disorder were excluded from study. The pre-anaesthetic evaluation was done one day prior to surgery. Patients were informed about the procedure and written informed consent was obtained from all the patients before surgery. Patients were randomly assigned to one of two groups, using a computer generated randomization table. In Operation room; they were connected to ECG, Peripheral oxygen saturation (SpO2) and Non-invasive blood pressure (NIBP). Intravenous line with 20G cannula was secured in the preparation area. Both pre-treatment drugs were stored at room temperature (20–23C) and prepared in 1ml syringe. Patients were given Intravenous Ringer lactate fluid in the dose of 7ml/kg/hr for fasting interval and was continued as maintenance fluid in the dose of 4ml/kg/hr. The investigator gave study drug, either 15mg [E15] or 30mg[E30] of injection ephedrine(1ml) deep intramuscular, 10 minutes prior to subarachnoid block. In operation room, under sterile preparation, patients were given spinal anaesthesia in sitting position with no. 26 spinal needle and 3 ml of 0.5% Bupivacaine heavy was given intrathecally. Patients were made supine immediately. The segmental level up to T6 was checked with pin prick method and the surgery commenced. Systolic arterial pressure (SAP) Mean arterial pressure (MAP) and pulse rate(HR) were noted; before spinal anaesthesia, and after spinal anaesthesia at 5 and 10 minutes interval and thereafter every 10 minutes, till 60 minutes. Any untoward event was noted if present. Injection Midazolam 1 mg was given intravenous (IV) as sedation if needed. Statistical Analysis: Few of our references studied earlier [10] along with Confidence Interval (CI) of 95% and p value <0.05, we had conducted a pilot study on 20 patients. Using this information, we could get sample strength of 35 patients in each group with two sided α-error of 5% and power study to be >80%. To compensate for potential dropout, 60 patients (30 per group) were considered necessary. Continuous variables were represented as mean values with standard deviation or frequency. Categorical variables were described as n (%) Demographic data like Age, Sex, and ASA-PS were analyzed using Chi-square test. Rescue ephedrine doses were analyzed by Mann Whitney U test. For all results P value <0.05 were considered significant. Statistical analysis was performed using unpaired 2 tailed student’s t test and regression analysis as appropriate with SPSS (Statistical Package of Social Sciences) version 20.0 software.
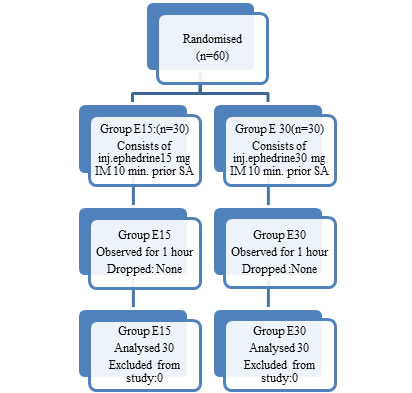
RESULTS Study included 60 patients (n=30/group). A flow chart is shown in [Figure 1]. Demographic data and clinical characteristics of patients are presented in [Table 1]. Data regarding percentage (%) change in Systolic Arterial Pressure is shown in [Table 2]. Percentage (%) change in Mean Arterial Pressure is shown in [Table 3]. Variations in Heart Rate are shown as percentage (%) in [Table 4]. Intravenous consumption of rescue doses of injection ephedrine are shown in [Table5] Figure 1: Flow Chart
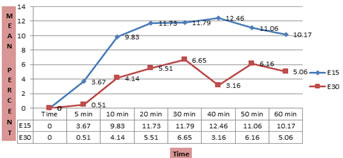
SAP was maintained with [E30] group without significant percentage change (mean 0-5%) in comparison to [E15] group (mean 0-10%). At 40 minutes interval percentage change in [E30] group was significantly minimal (mean 3.16%).[Table 2]. Intraoperative Systolic Blood pressure [Table2] and Mean arterial Pressure [Table3] had overall trend to decrease values during the procedure. However there is rise in HR with [E30] group at 30, 40, 50 minutes [Table 4] (P value<0.05) Intravenous ephedrine consumption in aliquots of 5mg was: Ten doses in [E15] group and six doses in [E30] groups [Table5]. Fewer patients in [E30] group had ventricular arrhythmia while nausea-vomiting was occasional in [E15] group Postoperatively, the hemodynamic parameters like SAP, MAP and HR were stable in both the groups for six hours. The two groups were comparable in the categorical variables like Age, Gender, ASA-PS and Duration of surgery [Table 1]. The number of male patients was higher than females in each group showing no statistical significant difference (P >0.05)
Table 1: Demographic Profile
Table 2: Comparison of severity of % change in Systolic Blood Pressure (SAP) between two groups at various time intervals with baseline systolic Arterial Pressure
Data described as (mean±SD) ; n=number ; * P<0.05 is significant.
Figure 2: Graphical representation of Percentage SAP Change
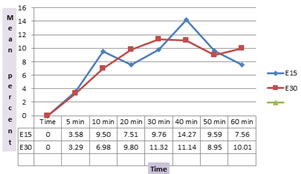
Table 3: Comparison of severity of % change in Mean Arterial Blood Pressure (MAP) between two groups at various time intervals with baseline Mean Arterial Blood Pressure
Figure 3: Graphical representation of Percentage MAP Change
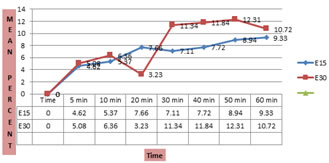
Table 4: Comparison of severity of % change in Heart rate between two groups at various time intervals with baseline heart rate
Figure 4: Graphical representation of Percentage HR Change
Table 5: Number of administered rescue doses of ephedrine (IV injection ,5mg /dose) after spinal anaesthesia; during 1 hour (Total)
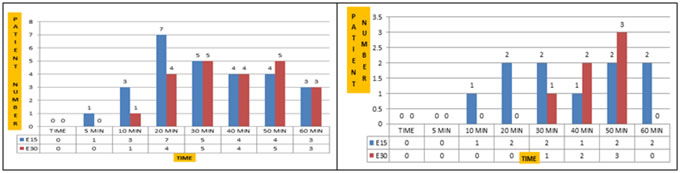
SAP, MAP and HR were recorded before giving spinal anaesthesia, 5 minutes after anaesthesia and thereafter every 10 minutes till 60 minutes. All measurements were obtained from upper arm with NIBP monitoring. A reduction of SAP>30%from the baseline level was considered negative outcome in terms of efficiency. Whereas increase in SAP> 20% and HR>20% were considered as adverse reaction. Figure 5: Graphical representation of 20% SAP Change Figure 6: Graphical representation of 25% SAP Change OBSERVATUONS Study 1: The systolic arterial blood pressure (SAP) was recorded in both the groups at 5minutes, 10 minutes and thereafter every 10 minutes till 60 minutes. SAP was maintained with [E30] group without significant percentage change (mean 0-5%) in comparison to [E15] group (mean 0-10%). At 40 minutes interval percentage change in [E30] group was significantly minimal (mean 3.16%). [Table2] Study 2: Approximately 20% of SAP fall from baseline was seen in almost all the patients in both groups at 30, 40 and 50 minutes intervals. This was more pronounced at 40 minutes interval with [E15] group compared with [E30] group (P=0.02). Study 3: Ten patients in [E15] group had approximately 25% fall in SAP (33% patients) while five patients (16.6% patients) had similar fall in [E30] group Study 4: Four patients out of 30 in [E15] group required rescue dose of Inj. Ephedrine (Total 10 doses) while three patients out of 30 in [E30] group required rescue inj. Ephedrine (Total 6 doses) in 1 hour to maintain blood pressure within range without adverse effect. (P =0.11))
DISCUSSION Ephedrine is indirectly acting sympatho-mimetic amine which increases alpha and beta receptor activities. Its main action is on beta1adrenergic receptor of the heart which increases heart rate and stabilizes blood pressure.3 Though crystalloid preloading is commonly practiced measure to avoid hypotension following spinal anaesthesia; it cannot be guaranteed by such measure alone or by routine conventional measures. There were many studies in the past which assessed the efficacy of IM inj. Ephedrine as a prophylactic use to prevent hypotension following spinal anaesthesia, but none of them analysed the proper dose regime, compared to its time interval of administration. Varathan S, Ekanayake SU, Amarasinghe U. et al.10 found out that in pregnant parturient combination of preloading with prophylactic IM injection Ephedrine is more effective and demonstrated that 15mg dose of injection Ephedrine given 10 minutes prior to spinal anaesthesia reduced hypotension and maintained better hemodynamic stability during elective caesarean sections. Sternlo JE, Rettrup A, Sandin R.et al.11Mentioned that volume expansion alone with colloid or crystalloid has not been effective for avoiding hypotension induced by spinal or extradural anaesthesia. It may be sometimes harmful in elderly patients with incipient heart failure conditions. As hypotension may develop rapidly after spinal anaesthesia, optimal SAP control with these techniques calls for very closely monitoring by invasive or automated techniques which are not always feasible. They have concluded that IM 0.6mg/kg dose of Injection Ephedrine was appropriate and reliable regime when injected deep intramuscularly into paravertebral muscles. That regimen provided a significant stabilizing effect on SAP throughout the study period of one hour. This effect was seen both with the hypertensive patients on Calcium channel or beta blockers medications. Hemmingsen C, Poulsen JA, Risbo A.et al.12 used prophylactic Injection Ephedrine 12.5mg IV and 37.5mg IM route in ASA I-III patients and concluded that prophylactic ephedrine was desirable for spinal anaesthesia, especially in ASA III patients. In our study, we have chosen patients from 18-65 age groups of both genders with exclusion criteria, posted for elective surgeries lasting for 1 to 2 hrs without any co-morbid diseases. We have prophylactically used Injection Ephedrine in the dose of 15mg or 30mg, deep intramuscularly 10 minutes prior to subarachnoid block for various surgical, gynaecological and orthopaedic procedures with varying duration. After taking care of their fasting period fluid requirements we found out that SAP was maintained to threshold level with [E30] group without significant percentage (%) change. There was rise in Heart rate at 10, 30, 40 and 50 minutes interval in [E30] group (P<0.05) It never exceeded to >20% from baseline heart rate. Mean Arterial Pressure was significantly low at 20 minutes interval with [E15] group compared to [E30] group (P=0.05) In current study we have achieved hemodynamic stability; avoiding hypotension following subarachnoid block with varying success ,with intramuscular (IM) injection Ephedrine in 30mg dose, compared to 15mg dose, given 10 minutes prior to spinal anaesthesia, without any adverse outcome.
CONCLUSION To conclude Injection Ephedrine in the dose of 30mg given via intramuscular route, 10 minutes prior to spinal anaesthesia, may be suitable fixed prophylactic dose to prevent hypotension following subarachnoid block.
ACKNOWLEDGEMENT I sincerely acknowledge my gratitude to Dr. Swati Raje; who helped in statistical analysis for this study. I acknowledge all my participated patients who allowed to conduct the study and gave informed consent accordingly. I am thankful to members of Ethical Committee of MIMER Medical College, Talegaon Dabhade, Pune, who permitted me to pursue my research.
REFERENCES
Policy for Articles with Open Access: Authors who publish with MedPulse International Journal of Pediatrics (Print ISSN: 2579-0897) (Online ISSN: 2636-4662) agree to the following terms: Authors retain copyright and grant the journal right of first publication with the work simultaneously licensed under a Creative Commons Attribution License that allows others to share the work with an acknowledgement of the work's authorship and initial publication in this journal. Authors are permitted and encouraged to post links to their work online (e.g., in institutional repositories or on their website) prior to and during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work.
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.