 Home
Home
|
Table of Content - Volume 19 Issue 3 - September 2021
The effect of perioperative magnesium sulphate on the total anesthetic and analgesic requirement in neck surgery
Krupa R Patel1*, Vandana Parmar2, Urmi Dave3
1Senior Resident, 2Professor & HOD, 3Assistant Professor, Department of Anaesthesiology, P.D.U. Government Medical College and Hospital, Rajkot-360001, INDIA. Email: dr.krupa1212@gmail.com
Abstract Background: The major perioperative goal is to provide adequate depth of anaesthesia along with optimum perioperative analgesia. One of the IV adjuvant that has been shown potential in pre-emptive analgesia is magnesium sulphate. This study was designed to assess the effect of perioperatively administered IV magnesium sulphate on anaesthetic and analgesic requirements. Materials And Methods: Sixty patients of ASA class 1, 2, 18-65 years of age scheduled for neck surgeries were randomly divided in to two groups. Group M received 40 mg/kg, magnesium sulphate in 100ml normal saline as loading dose over 20min followed by 8 mg/kg/hour as infusion till the end of the surgery during total intravenous anaesthesia with propofol, fentanyl and atracurium in neck surgeries. Group C received 100 ml normal saline as loading dose over 20min and thereafter continuous infusion of same volume of normal saline as received by group M. We observed total requirement of inj.propofol and inj.atracurium intraoperatively and duration of postoperative analgesia in both the groups. Results: The mean VAS score was consistently high in Group C than group M during first 24 hours which was statistically significant (p<0.05). The mean duration of total analgesia was significantly higher in group M. And total requirement of propofol and atracurium in control group were significantly higher compared to group receiving Mgso4.Conclusion: Perioperative use of magnesium sulphate as preloading and infusion shows reduced analgesic and anaesthetic drugs requirements in neck surgeries. Key words: Analgesic effect, Magnesium Sulphate, Neck surgeries, Propofol, VAS score.
INTRODUCTION Postsurgical pain is one of the most important issues that could affect postoperative peace and comfort. Neck surgeries are associated with intense inflammatory response, resulting in moderate to severe postoperative pain perception.1–3 The major goal in postoperative pain management is to minimize the dose of medications and lessen side effects, while still providing adequate analgesia,4 Narcotics are the most common analgesics which are used after the surgeries. But anaesthetists are always looking for replaceable methods with fewer side effects and cost.2,3 It has been suggested that magnesium has the potential to prevent and treat pain by acting as an antagonist of N-methyl-d-aspartate (NMDA) receptors.5
MATERIAL AND METHOD We obtained approval from our institution’s ethics committee and written informed consent was obtained from patients. We recruited 60 patients of adult age group (15-65 year) of ASA status of I, II and III scheduled for neck surgeries. Group M: patients received 40 mg/kg , magnesium sulphate in 100ml normal saline as loading dose over 20minutes and 2 gm magnesium sulphate in 50 ml normal saline at the rate of 8 mg/kg/hour as infusion till the end of the surgery Group C: patients received 100 ml isotonic saline as loading dose over 20minutes and thereafter continuous infusion of same volume of normal saline as received by group M. All the patient were undergone a pre-anaesthetic checkup before surgery and all the routine and specific investigations have been documented. The patients were nil per oral for 6 hours before surgery. Standard monitors were applied including BIS monitor and nerve stimulator and patients’ baseline parameters like pulse, blood pressure, respiratory rate, spO2, BIS value had been recorded and monitored throughout the procedure. I.V. line of 20 gauge on both hands was secured. Patient were premedicated with Inj. Glycopyrolate (0.2mg) IV, Inj. Fentanyl 1.5-2 microgram/kg IV, Inj. Ondansetron (4mg) I.V. After preoxygenation with 100% oxygen for 3 minutes, anaesthesia was induced with Propofol 2 mg/kg and tracheal intubation facilitated by inj. Succinylcholine 1.5 mg/kg by I.V. route. Anaesthesia was maintained using controlled infusion of propofol 6-8 mg/kg/hour and titrated to maintain the BIS value within the range of 45-60. Neuromuscular blockade was achieved with atracurium 0.5 mg/kg as bolus and top up doses of atracurium 0.1 mg/kg was given when the TOF stimulations were more than two responses. Intra operatively surgical plane of anaesthesia was maintained by monitoring the BIS which was kept between 45 to 60.When BIS value was more than 60 propofol infusion rate increased from 8mg/kg/hour to 10 mg/kg/hour up to 12mg/kg/hour. Then after decresed to 8mg/kg/hour gradually if BIS value is less than 60.Changes in HR > 20% ,mean arterial pressure >20% above the base line for more than one minute when the BIS value is already in the range of 45-60, fentanyl top up of 10-20 mcg was given to adjust the hemodynamics. In case of any episode of bradycardia that was HR< 50beats /min and hypotension that is 80mmHg was managed with i.v. atropine 0.02mg/kg and i.v. mephentermine 0.1mg/kg respectively. Propofol and Magnesium sulphate infusions were stopped at the end of surgery. At the end of surgery all patients were reversed with inj. neostigmine 0.05mg/kg i.v. + inj. glycopyrolate 8mcg/kg i.v. Each patient was observed continuously after the termination of anaesthesia for any events. Pain was assessed by VAS score (1-10) at immediate postoperative period till 24 hours postoperative. Postoperative rescue analgesia was given with inj. diclofenac sodium 1.5mg/kg IV when VAS score was >3. Statistical analysis of data: The statistical analysis was done using site-http://www.Figurepad.com/quikcals/ttest/?Format=SD. Parameters [ Age, gender, mean arterial pressure, heart rate, VAS score, duration of analgesia, total requirement of propofol, total requirement of atracurium] were compared between two groups by unpaired t test. A p value less than 0.05 was considered statistically significant.
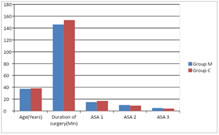
OBSERVATION AND RESULT This study was a prospective, randomized controlled study. 60 patients were enrolled 30 patients were taken in each group. These two groups were comparable in respect to demoFigureic variables (age, ASA grade II/III and duration of surgery.) [Figure 1]
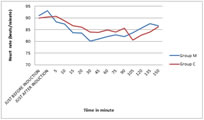
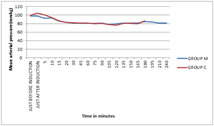
Figure 1: DemoFigureic data There was no significant difference in heart rate among both the group before induction, after induction and intraoperatively. (P >0.05)[Figure 2] There was no significant difference in mean arterial pressure among both the group before induction (p>0.05).The MAP increased in group C (104.68±5.59) as compared to group M (97.57±8.72) just after induction was statistically significant (p<0.05). After that there was no significant difference among both the groups till the end of surgery. [Figure 3] Figure 2: Intra operative heart rate (Beats/minutes)
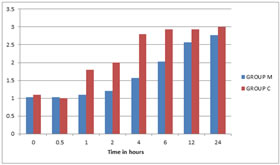
Figure 3: Intraoperative mean arterial pressure (mmhg) The mean VAS score was consistently high in group C than group M during first 24 hrs which was statistically significant (p<0.05).(Table 1, Figure 4) Table 1: VAS Score
S: significant (P value:≤0.05), NS: Not Significant (P value:>0.05), HS: Highly Significant( P value:<0.001)
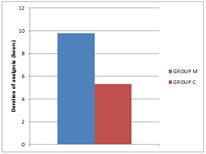
Figure 4: VAS score In group C mean duration of analgesia was 5.336±1.564 hours and in group M it was 9.766±1.381 hours. This analysis shows that mean duration of total analgesia was significantly higher in group M than group C. (p value 0.0001)(Table 2, Figure 5) Table 2: Duration of analgesia
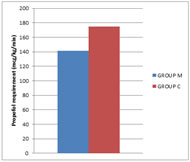
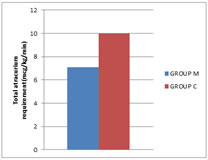
Figure 5: Duration of analgesia (hours) Total requirement of propofol in group M (0.141±0.0166 mg/kg/min)and group C (0.175±0.009 mg/kg/min). In Group C it was significantly higher than group M (P<0.05)(Table 3,Figure 6) Total requirement of atracurium in group M (0.0071±0.0008 mg/kg/min) and group C (0.010±0.001 mg/kg/min). In Group C it was significantly higher than group M (P<0.05)(Table 4,Figure 7)
Table 3: Total propofol requirement
Table 4: Total requirement of atracurium
Figure 6: Propofol requirement Figure 7: Total atracurium requirement(mcg/kg/min) In Group M two (6.66%) cases of PONV were reported and in Group C three (10%) cases of PONV were reported. Which was treated with inj.ondansetron. In Group M one (3.33) case of shivering was reported whereas in Group C two (6.66) cases of shivering were reported. Which was treated with inj.dexona.
Table 5: Complications and drugs Used
DISCUSSION One of the most important issues that could affect postoperative peace and comfort is postsurgical pain. Neck surgeries are associated with intense inflammatory response, resulting in moderate to severe postoperative pain perception1–3 The major goal in postoperative pain management is to minimize the dose of medications and lessen side effects4 So we studied effect of magnesium sulphate on the total anesthetic and analgesic requirement in neck surgery to explore the potential of magnesium sulphate to provide analgesia by its action on NMDA receptor and its potential to prolong neuromuscular blocking effect by its action on neuromuscular junction. We studied 60 patients (age between 15 and 65 years) of ASA grade I,II and III undergoing elective thyroid surgeries under general anaesthesia, we randomly allocated patients in 2 groups, Group M (Magnesium sulphate) and Group C (Control). The primary aim of this clinical study was to evaluate the effect of perioperative magnesium sulphate on the total anaesthetic and analgesic requirement in neck surgeries. Both the groups were comparable for demographic data and no statistically significant difference were found between groups regard to age and gender. L.telci et al.6 studied effects of magnesium sulphate in reducing intraoperative anesthetic requirements and Martin R et al.8 studied role of magnesium sulfate in postoperative analgesia both found no significant differences in the age, weight, height, the length of surgery and the length of anesthesia. There was no significant difference in heart rate among both the group. Just after induction (approximately coinciding with the time of intubation) increase in heart rate was more in group C as compared to group M but the difference was statistically insignificant (p>0.05). Similar to our study J-H Ryu5 studied effects of magnesium sulphate on intraoperative anaesthetic requirements and postoperative analgesia in gynaecology patients receiving total intravenous anaesthesia. There was no statistically difference in heart rate between the two groups.(P>0.05).Martin R tramer et al.7 studied role of magnesium sulfate in postoperative analgesia and found no significant difference in intraoperative heart rate. There was no significant difference in mean arterial pressure among both the group before induction (p>0.05). The MAP increased in group C (104.688±5.5955) as compared to group M (97.5777±8.7283) just after induction and after 5 minute was statistically significant (p<0.05). The MAP was insignificant among the two groups till the end of the surgery. Significant reduction in blood pressure in group M compared to group C just after induction and 5 minutes after induction which nearly matched laryngoscopy and tracheal intubation period may suggest that magnesium sulphate attenuates response to laryngoscopy and tracheal intubation. Our study correlated with Arman Taheri et al.8 who studied on effect of low-dose (single-dose) magnesium sulfate on postoperative analgesia in hysterectomy patients receiving balanced general anesthesia and found no significant difference in heart rate and arterial blood pressure. Martin R tramer et al.7 studied role of magnesium sulfate in postoperative analgesia and found no significant difference in intraoperative mean blood pressure. The mean VAS score was consistently high in group C than group M during first 24 hrs which was statistically significant (p<0.05). J H Rhyu et al.5 studied on effects of magnesium sulphate on intraoperative anaesthetic requirements and postoperative analgesia in gynaecology patients receiving total intravenous anaesthesia. They found that VAS score was significantly lower in magnesium group as compared to saline group. Sara Asadollah et al.9 studied the effect of magnesium sulphate on postoperative analgesia requirements in gynecological surgeries. In their study the patients in control group showed higher postoperative pain on average on VAS in comparison with study group at the end of 30 min, 4 hours and 12 hours. In our study, in group C mean duration of analgesia was 5.336±1.564 and in group M it was 9.766±1.381 hour. This analysis shows that mean duration of total analgesia was significantly higher in group M than group C. (p value <0.001).This study demonstrates that magnesium sulphate potentiates postoperative analgesia. Similar to our study IH Koinig et al.10 who studied whether magnesium sulfate reduces intra- and postoperative analgesic requirements, Sara Asadollah et al.9 studied the effect of magnesium sulphate on postoperative analgesia requirements in gynecological surgeries and concluded that magnesdium sulphate increases duration of analgesia. Total requirement of propofol was significantly lower (P value< 0.001) in group M (0.141±0.0166 mg/kg/min) compared to group C (0.175±0.009 mg/kg/min). Total requirement of atracurium was significantly lower(P value< 0.001) in group M (0.0071±0.000845mg/kg/min) compared to group C (0.010±0.001 mg/kg/min). Magnesium prolongs and potentiates neuromuscular block by non-depolarizing neuromuscular blocking agents by acting as a calcium channel blocker at presynaptic nerve terminals and decreases acetylcholine release at the motor endplate, which diminishes muscle fiber excitability and reduces the amplitude of endplate potential. However, this effect of magnesium sulphate did not prolong emergence from in the present study probably because neuromuscular transmission was monitored throughout the study and additional doses of atracurium were administered using a strict criterion, a TOF count of 2 or greater. Unlike inhalation anaesthetics, propofol has no potentiating effect on neuromuscular blocking agents and therefore magnesium sulphate may be a useful adjunct in surgery that requires adequate muscle relaxation.L.telci et al.6 studied evaluation of effects of magnesium sulphate in reducing intraoperative anesthetic requirements and found that significantly lower propofol, remifentanil and vecuronium requirements were recorded during each measurement. Sara Asadollah et al.9 studied the effect of magnesium sulphate on postoperative analgesia requirements in gynecological surgeries and found that use of perioperaayive magnesium sulphate decreases total requirements of propofol and muscle relaxants. In Group M two cases of PONV were reported and in Group C three cases of PONV were reported. In Group M one case of shivering was reported whereas in Group C two cases of shivering were reported. This complications were not much significant and were not related to the study drug. Sara Asadollah et al. 9 studied on effect of magnesium sulphate on postoperative analgesia requirements in gynecological surgeries in their study incidence of nausea or vomiting were similar in both the groups. Kiran S et al.11 studied evaluation of a single-dose of intravenous magnesium sulphate for prevention of postoperative pain after inguinal surgery in their study incidence of nausea or vomiting were similar in both the groups.
CONCLUSION From this study we concluded that perioperative use of magnesium sulphate preloading with 40mg/kg and intraoperative infusion of 8mg/kg/hr attenuated nociceptive stimulation by its action as NMDA receptor antagonist and a calcium channel blocking action which can be proved by reduced analgesic requirements. (Figure No.7) By use of magnesium sulphate there was decreased requirement of anesthetic drugs(Figure No.9) as magnesium acts as a calcium channel blocker at presynaptic nerve terminals and decreases acetylcholine release at the motor endplate, which diminishes muscle fiber excitability and reduces the amplitude of endplate potential, resulting in the potentiation of a neuromuscular blockade by nondepolarizing neuromuscular blocker.
REFRENCES
Policy for Articles with Open Access
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.