 Home
Home
|
Table of Content - Volume 20 Issue 1 - October 2021
Comparative study of Midazolam and Nalbuphine with Midazolam and Fentanyl for respiratory effect in patients undergoing FESS under Mac
Comandur Lavanya
Associate professor, Department of Anaesthesia, Viswabharathi Medical College, Kurnool, INDIA. Email: lavcom13@yahoo.co.in
Abstract Background: Functional Endoscopic Sinus Surgery (FESS) is a procedure for surgical management for chronic sinusitis. Present study was conducted to compare the Midazolam and Nalbuphine with Midazolam and Fentanyl for respiratory effect in patients undergoing Fess under MAC at tertiary care hospital. Materials and Methods: Present study was a prospective, comparative and randomized study, conducted in patients of either gender, above 18 years of age, belonging to ASA-I/II, scheduled for elective surgery and willing to participate. 100 patients were randomly allocated into two groups group N and group F of 50 patients each by using chit and box method of randomization. Group N patients were given intravenous inj. Nalbuphine and group F patients were given intravenous inj. Fentanyl. Parameters like respiratory rate, SpO2, RSS and the number of patients requiring supplemental O2 were compared in both the groups. Results: In present study total 100 patients were studied. 50 patients each were allocated to each group (group F and group N). General characteristics such as age, gender, height, weight, ASA status were compared in both groups and difference was not statistically significant. Parameters like respiratory rate, SpO2 and RSS were compared in both groups and difference was statistically significant. Number of patients requiring supplemental oxygen was more in Fentanyl group. Conclusion: Nalbuphine -Midazolam combination proved to be superior compared to Fentanyl- Midazolam combination as it produces less respiratory depression and provided better patient comfort. Keywords: FESS, Midazolam, Nalbuphine, Fentanyl, Ramsay sedation scale,
INTRODUCTION FESS (functional endoscopic sinus surgery) is a surgical treatment of long-standing sinus infections. Surgeon uses endoscopy in the nose to view the sinuses and do surgery. The important problem involved in surgery is small space and continuous bleeding from sinuses as the sinuses have rich supply of blood. The sinuses are surrounded by important organs like eyes and brain, so good surgical skill is utmost important to the surgeon for success in doing FESS surgery.1 This surgery can be done under general anaesthesia or local anaesthesia with Monitored Anaesthesia Care (MAC). General anaesthesia is time consuming, not cost effective and is associated with many complications. MAC involves administration of local anaesthesia combined with IV sedation, anxiolytics and or analgesic drugs. The ideal anaesthetic method should be non-invasive, short, cheap and comfortable for patient and surgeon. Good patient selection, pre-operative counseling and use of appropriate sedation are important factors for success of septoplasty under local anaesthesia.2 Several drugs have been used for sedation during surgical procedure under monitored local anaesthesia including propofol, benzodiazepines and opoids.3 But these drugs are associated with increased risk of over sedation and respiratory depression which makes these drugs less than ideal.4 Dexmedetomidine is a highly selective alpha 2 adrenoreceptor agonist which has both sedation and analgesic effect without inhibiting respiration.5 So the present was done to compare the Midazolam and Nalbuphine with Midazolam and Fentanyl for respiratory effect in patients undergoing FESS UNDER MAC at tertiary care hospital.
MATERIALS AND METHODS This prospective, comparative and randomized study was conducted from January 2019 to December 2019 at the department of anaesthesia, Viswabharathi Medical College and General Hospital, Kurnool, Andhra Pradesh after obtaining approval from Institutional ethics committee. 100 patients belonging to ASA physical status I and II and above 18 years of age irrespective of sex, height and weight were selected for elective FESS. Informed written consent was taken from participants in the study. Exclusion criteria included patients allergic to local anaesthetics and opiods, patients belonging to ASA grade III and IV with morbid symptoms, patients suffering from bleeding disorders, patients having oxygen saturation (SpO2) <90 and pulse rate <60. 100 patients were divided into 2 groups group F and group N consisting of 50 patients each. Group F received Midazolam-Fentanyl combination while group N received Midazolam -Nalbuphine combination. On the morning of surgery, the patient was counseled regarding the technique of anaesthesia being given as local anaesthesia with sedation. Intravenous line was secured with No.20 iv catheter. One bottle of dextrose saline was started slowly. Inj. Ondansetron 0.2mg/kg along with an intravenous antibiotic of surgeries choice was given. Monitors were connected and baseline parameters were recorded i.e. O2 saturation, respiratory rate and level of conscious by RSS. The patient then received injection glycopyrolate 0.2mg. following this group F received inj. Midazolam 0.08mg/kg with a ceiling dose of 3mg and injection Fentanyl 2µg/kg with a ceiling dose of 100µg. group N received Inj. Midazolam 0.08mg/kg with a ceiling dose of 3mg and inj. Nalbuphine 0.3mg/kg with a ceiling dose of 20 mg. The injections were given slowly over a period of 3 minutes. Simultaneously the surgeon was asked to give local anaesthesia at the site of injury with 2% lignocaine with adrenaline. At the end of 3 minutes, the following parameters were measured at an interval of 2 min up to 10 minutes followed by 15 min, 20 min, 25 min and 30 min respectively
The study ended at 30minutes, as most cases of FESS are completed within 30 minute time. In this Blood Pressure was not monitored as its effect was masked by adrenaline given by the surgeon at the surgical site. Supplemental Oxygen was not given in the beginning of the study as it will mask the measurement of Oxygen saturation in both the groups. But supplemental Oxygen was given when the saturation dropped below 85.Tthe number of patients requiring supplemental Oxygen was compared in both the groups. The data was analyzed using SPSS version 16 and Microsoft Excel. Descriptive statistics was done for all data and reported in terms of mean and percentages. Continuous variables were analyzed by t test. Categorical variables were analyzed with the help of chi square test. Statistical significance was taken as p<0.05.
RESULT In present study total 100 patients were studied. 50 patients each were allocated to each group (group F and group N). General characteristics such as age, gender, weight, and ASA grade were compared in both groups and difference was not statistically significant. Table 1
Table 1: General characteristics:
Parameters like Respiratory rate, SpO2 and Ramsay sedation scale were compared in both groups. Normal respiratory rate varied between 12-16/min. but in our study, all patients had preoperative baseline respiratory rate varying between 16-24/min. this may be due to 2 reasons;
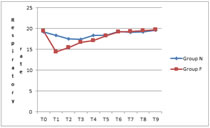
Respiratory rate was compared between the two groups from baseline at different intervals of time. In the Fentanyl group, the respiratory rate was lower at 2 minutes, 4 minutes, 6 minutes and 8 minutes which was statistically significant. Table 2 and Fig 1 Table 2: Group comparison of mean respiratory rate from baseline at different intervals of time
Figure 1: Compare of mean respiratory rate between the two groups
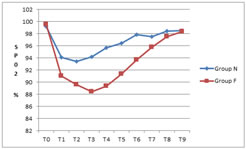
SpO2 was compared between the two groups from baseline at different intervals of time. In the Fentanyl group, the SP02 was lower at 2 minutes, 4minutes, 6 minutes, 8 minutes,10 minutes, 15 minutes, 20 minutes and 25 minutes which was statistically significant. It was observed that in Fentanyl group 13 out of 50 patients required supplemental oxygen and none of the patient in Nalbuphine group required supplemental oxygen Table 3 and Fig 2 Table 3: Group comparison of Mean SpO2 from baseline at different intervals of time
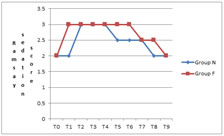
Figure 2: Comparison of SpO2 between the two groups Ramsay Sedation Score (RSS) was compared between the two groups from baseline at different intervals of time. In the Fentanyl group, the RSS was more at 2 minutes, 10 minutes, 15 minutes, and 25 minutes which was statistically significant. Table 4 and Fig 3 Table 4: Group comparison of Mean Ramsay Sedation Score (RSS) from baseline at different intervals of time
Figure 3: Comparison of Ramsay Sedation score (RSS) between the two groups
DISCUSSION This study was designed to compare the efficacy of Midazolam and Nalbuphine with Midazolam and Fentanyl for respiratory effect in patients undergoing FESS under MAC. The statistically significant differences observed in respiratory rate, Sp02, and Ramsay Sedation Score confirm that Fentanyl may cause greater respiratory depression than Nalbuphine at the doses used in this study. Fentanyl, a potent, short-acting opioid agonist, is a widely used pain-killer during short surgical procedures and however, the major worry to clinicians is that the utility of fentanyl has been noted to be quite narrow in comparison of its plasma levels between effective analgesia and significant respiratory depression.7-10 Nalbuphine is a 6-transmembrane MOR agonist as is buprenorphine and butorphanol all of which have a ceiling on respiratory depression.11 Nalbuphine is an opioid agonist–antagonist, active on mu and kappa receptors12 to provide analgesia and certain anti-pruritic effects13 and have less undesirable outcomes. The statistically significant low average SpO2 level and slow RR in Fentanyl group indicated that Fentanyl causes greater respiratory depression than Nalbuphine . The more frequent and marked episodes of hypoxemia observed in the Fentanyl group also support this finding. Our study showed that none of patients developed hypoxemia in Nalbuphine group vs. 13 patients developed hypoxemia in Fentanyl group. One study has found that Nalbuphine, as high as 0.8 mg/kg, will not aggregate respiration depression.13
CONCLUSION The results of this study confirm that Nalbuphine -Midazolam is effective than Fentanyl-Midazolam in FESS under MAC procedure as it produces less respiratory depression. Nalbuphine can be considered a safer alternative to Fentanyl in patients with respiratory problems.
REFERENCES
Policy for Articles with Open Access
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.