 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content Volume 10 Issue 3 - June 2019
Study of an outbreak of respiratory diphtheria in local community, Kakinada
R Usha Rani1, K R L SuryaKirani2*, A Durga Rani3
1Assistant Professor, Department of Microbiology, Mahavir Institute of Medical sciences, Vikarabad, Telangana, INDIA. 2Professor & HOD, 3Assistant Professor, Department of Microbiology, Rangaraya Medical College, Kakinada, Andhra Pradesh, INDIA. Email: ramavathusha@gmail.com
Abstract Objectives: 1. Isolation, speciation and toxigenicity testing of Corynebacterium diphtheria. 2. To study the epidemiology, clinical features, complications and outcomes in respiratory diphtheria. Materials and Methods: 31 suspected Diphtheria cases admitted in the G G H, Kakinada, were included in the study. Isolates identified by standard methods and toxigenicity by Elek's Gel Precipitation test. Isolates were sent to NICD for confirmation. Results: Out of 31 suspected cases of diphtheria, 8 were smear positive, 10 culture positive, 7 smear plus culture positive. Isolated strains were non toxigenic strains of Corynebacterium diphtheriae. gravis. In smear negative cases, Streptococcus pyogenes6, Staphylococcus aureus(4) were isolated. Clinical features were Fever in 18 cases, dysphagia 7, sore throat 5, Swelling of neck 7, Dyspnoea 3, greyish membrane over tonsils 9, Myocarditis 4, respiratory compromise in 6 cases. Death occurred in 10 cases. None had adequate immunization. Unknown history in 27 cases, first dose given in 2, first 3 doses given in 1, 1st booster dose given in 1 case.90% were from lower socio economic groups. First outbreak occurred in Fisherman community, Yetimoga, Kakinada. Survey was done in the area, Source could not be traced .12, 405 children below 10 years were immunized Chemoprophylaxis was given to all contacts. Conclusion: Poor immunization and lower socioeconomic status have resulted in an outbreak. Increased immunization coverage, early availability of ADS, early recognition and effective treatment could have reduced the incidence and mortality. Key Word: respiratory diphtheria. INTRODUCTION Diphtheria is a fatal disease and may cause serious complications if not recognized early and treated properly1. It is an acute infectious disease of the childhood characterized by local inflammation of the epithelial surface, formation of a membrane and severe toxemia.2 Caused by - Gram positive bacilli, Corynebacterium diphtheriae which is aerobic, non motile, non sporing3.Nearly one lakh cases of diphtheria were reported by WHO in 1980 and only 12735 cases in 2005 out of which nearly 80% were from India.2834 in 2006,3354 in 2007, 6081in 2008,according to the National Health Profiles released by the Central Bureau of Health Intelligence under the Directorate General of Health Services. WHO – 2525 in 2012.
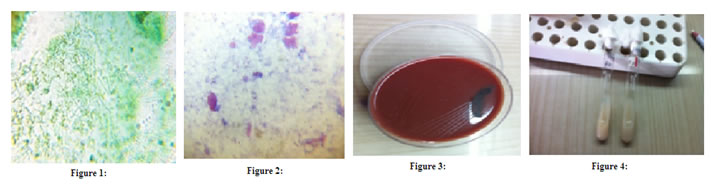
METHODOLOGY 31 patients identified as probable cases of diphtheria admitted at PICU and ENT, Government General Hospital, Kakinada from July–October 2013. Throat swabs were taken and processed according to the standard methods4. Immunization status, clinical features, complications and outcomes were noted. 3 throat swabs were collected, from the grayish membrane. With one swab, Albert staining, Gram Staining and Methylene Blue staining was done. Other swab was used to streak on Loffler's Serum Slope and Potassium Tellurite Blood Agar Plate. Third swab was inoculated on sheep blood agar5. Figure 1: Sample Collection, grayish Pseudomembrane Direct Smears
Figure 1: Alberts Stain; Figure 2: Grams stain; Figure 3: Growth on Potassium Tellurite; Figure 4: Growth On Loefflers Serum slope;
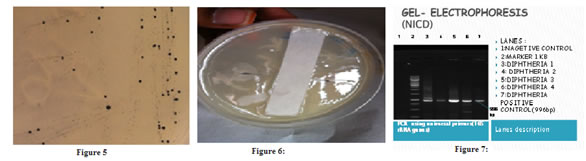
Figure 5: Growth On Tinsdale Agar devoid of blood; Figure 6: Elek’s Gel Precipitation Test; Figure 7: Gel-Electrophoresis
Out of 10 culture positive cases, 3 cases have been recovered with antitoxin and discharged home with Erythromycin 500mg bd for 7 days and followed up. 7 cases of culture positives, and 3 cases of late admission expired even after administration of antitoxin. 4(32.6%) developed myocarditis as evidenced by ECG.1(3.2%) child developed palatal palsy at the end of 1ST week. Death occurred in 10 patients, complications being Myocarditis and respiratory insufficiency. Of the 10 cases expired, 8 cases received antitoxin and 2 children expired before the initiation of DATS.
RESULTS Clinical Features
Table 1: Comparison with other studies
Table 2: Toxigenicity comparison with other studies
DISCUSSION Four isolates are Corynebacterium diphtheriae-gravis. Maltose, glucose and starch were fermented and Urease test was negative. Elek’s Gel precipitation test was done which did not show any precipitation lines. Hence, the isolates are non toxigenic strains of Corynebacterium diphtheriae. Followup of outbreak: Notified to the district authorities for further action. 90% were from lower socio economic groups, occurred in Fisherman community, Yetimoga, Kakinada. Survey was done in the area. Source could not be traced.12, 405 children below 10 years were immunized. Chemoprophylaxis(Erythromycin 500mg bd) was given to all contacts.
CONCLUSION Poor immunization and lower socioeconomic status have resulted in an outbreak. Though the isolates were non toxigenic strains of C. diphtheriae-gravis, fatalities occurred with complications. Early administration of ADS could have saved some cases. Early recognition and effective treatment could have reduced the incidence and mortality. Recommendations for prevention of re-emergence of Diphtheria: To inform the public and parents of young children of the hazards of diphtheria and the importance of immunization. Every membranous tonsillitis should be considered as diphtheria unless proved otherwise. Early diagnosis and treatment of cases. All cases, suspected cases, carriers should be isolated. Carriers should be treated with 10 days course of oral erythromycin. Prompt reporting to the authorities for further action.
REFERENCES
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||

 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.