A study of Candida species from vaginal discharge specimens of clinically symptomatic women of reproductive age group
Prabha Anand1*, Chaya A Kumar2, Sujata Baveja3
Department of Microbiology, Lokmanya Tilak Municipal Medical college, Sion, Mumbai, Maharashtra, INDIA.
Email: prabha.14.anand@gmail.com
Abstract Background: Candida species are part of the lower genital tract flora of healthy asymptomatic women. They eventually become pathogenic under some prevailing conditions. Confirmation of yeast species helps to initiate early appropriate antifungal therapy thereby reducing the morbidity. Aim: To isolate and identify Candida species from vaginal discharge specimens of clinically symptomatic women of reproductive age group. Material and Methods: From 184 symptomatic women, two high vaginal swabs were collected from posterior vaginal wall with aseptic precautions. First swab was used for microscopic examination. Second swab was used for fungal culture on Sabouraud’s dextrose agar (SDA) slant. Any growth suggestive of yeast was subjected to the CHROM agar test, corn meal agar test, germ tube test, urease test and sugar assimilation test as per standard protocol for further identification. Results: Out of the total 184 high vaginal swab specimens, Candida species was isolated in 42 cases (22.8%). Significantly higher percent of cases showed C.albicans 52.4%, followed by C. tropicalis 35.7%, C. krusei 7.1% and C. glabrata 4.8%. Conclusion: Candida albicans predominated in this study. Presumptive identification followed by confirmation of yeast species helps in initiating an early and appropriate antifungal therapy thereby reducing the morbidity.
Key Word: symptomatic women, vaginal discharge, Candida species, Candida albicans
INTRODUCTION
Vulvovaginal candidiasis (VVC) is a fungal or yeast infection of lower genital tract of the female caused by Candida species. This can be referred to as Candidiasis or Moniliasis. Candida species are part of the lower genital tract flora in 20%–50% of healthy asymptomatic women.1They are normal flora of the vagina that eventually become pathogenic under some prevailing conditions, and thus presents as a common etiology of vulvovaginitis. When prompt recognition and laboratory confirmation is not achieved, this could lead to devastating genital discomfort and a major reason for frequent hospital visits.1 Candida albicans is the most common species causing VVC. Neverthless, over last few years research evidence has demonstrated an increment in frequency of cases caused by non- albicans Candida species which could be due to indiscriminate usage of antimycotics which eliminates the more sensitive C.albicans.1 Diagnosis of VVC based only on patient history and genital examination is not possible because of the low specificity of symptoms and signs, since other causes like leukorrhea and pruritus vulvae, mimic VVC. Therefore, in order to have a definitive diagnosis of VVC, cultural isolation and identification of Candida spp. are crucial.1 Confirmation of yeast species helps to initiate early appropriate antifungal therapy thereby reducing the morbidity. Thus, the present study was carried out to isolate and identify Candida species from vaginal discharge specimens of clinically symptomatic women of reproductive age group.
MATERIAL AND METHODS
This prospective cross-sectional study was carried out in Department of Microbiology at a tertiary care hospital over a period of one and a half year. The study commenced after Institutional Ethics Committee approval.
Sample size: Sample size was calculated by the Absolute Precision Formula: Sample size (n) = Z2 X PQ/d2Where,
a) P=prevalence,
b) Q=100-P,
c) Confidence level=95%, therefore Z = 2,
d) Absolute precision required on either side of the proportion (in percentage points) d=10 percentage points i.e. 10% confidence interval. Thus, a total of 184 women from reproductive age group were included in the study.
Inclusion criteria
• Women in 15 to 45 years age group with symptoms of vaginal discharge with or without itching around the vaginal region or erythema or pain.
• Women who were sexually active.
Exclusion criteria
• Women with history of local or systemic antifungal treatment in the past one month.
• Pregnant women with medical disorders.
• Women who have never been sexually active.
• Women currently menstruating.
• History of hysterectomy.
A detailed clinical history was taken from the patients regarding age, use of contraception, associated comorbid conditions like diabetes, infertility, pelvic inflammatory disease and previous history. Following clinical examination, two high vaginal swabs were collected from posterior vaginal wall with aseptic precautions and sent to Microbiology department for further processing.
Processing of the sample: First swab was used for microscopic examination. Wet mount and smear for Gram staining was prepared from this swab as per standard protocol. Second swab was used for fungal culture. It was streaked on both Sabouraud’s dextrose agar (SDA) slant with chloramphenicol and gentamycin and also on Sabouraud’s dextrose agar with chloramphenicol, gentamycin and cycloheximide. They were then incubated at 37°C and 25°C respectively for 4 weeks. These slants were examined for growth, daily for the first week and twice a week for subsequent period. Any growth suggestive of yeast was subjected to the CHROM agar test, corn meal agar test, germ tube test, urease test and sugar assimilation test as per standard protocol for further identification.2
Statistical analysis : Statistical analysis was performed with the software package: SPSS statistic 20 for Windows. The significance of difference of proportion of categorical variables among groups was examined by the chi-square test (large samples) and Fischer’s exact test (small samples). The difference in mean was examined by student’s t test. A value of P of </=0.05 was considered significant for all statistical analyses and is marked with an asterisk(*).
Out of the total 184 high vaginal swab specimens, Candida species was isolated in 42 cases (22.8%) while in the rest 142 (77.2%) specimens no fungal growth was seen. Thus the prevalence of VVC in the present study was 22.8%.
Table 1: Correlation of different age group with growth of Candida species
Age group |
Diagnosis |
Total |
Test |
P value |
Growth of
Candida |
No growth of Candida |
21-25yr |
Count |
2 |
10 |
12 |
Fischer’s Exact test value: 13.257 |
0.006* |
% |
16.7% |
83.3% |
100% |
26-30yr |
Count |
16 |
24 |
40 |
% |
40% |
60% |
100% |
31-35yr |
Count |
19 |
65 |
84 |
% |
22.6% |
77.4% |
100% |
36-40yr |
Count |
4 |
42 |
46 |
% |
8.7% |
91.3% |
100% |
41-45yr |
Count |
1 |
1 |
2 |
% |
50% |
50% |
100% |
Total |
Count |
42 |
142 |
184 |
% |
22.8% |
77.2% |
100% |
Mean age in years |
31.71±3.73 |
33.13 ±4.26 |
32.81 ±4.18 |
T= 3.797 |
0.053 |
Candida positive and negative cases were compared in various age-groups. Amongst various age groups, 26-30yr (40%) followed by 31-35yr (22.6%) and 21-25yr (16.7%) showed higher percent of Candida positive cases as compared to other age groups. This variation seen in culture positive cases over different age groups was found to be statistically significant. Mean ages of Candida positive and negative cases were compared. This was not found to be statistically significant. In 42.9% of cases both pus cells and yeast cells were seen on gram stain whereas in 57.1% cases, pus cells and yeast cells were not seen on gram stain. There was no significant difference seen on gram stain findings of pus cells and yeast cells.
Table 2: Distribution of Candida species in VVC cases
Species of candida |
No. of patients |
Percentage (%) |
C. albicans |
22 |
52.4 |
C. tropicalis |
15 |
35.7 |
C. krusei |
3 |
7.1 |
C. glabrata |
2 |
4.8 |
Total |
42 |
100 |
Cases positive for Candida were divided into groups based on the species isolated. Significantly higher percent of cases showed C. albicans 22 (52.4%) followed by C. tropicalis15 (35.7%). (Chi square value: 26.762; P value: <0.001*).
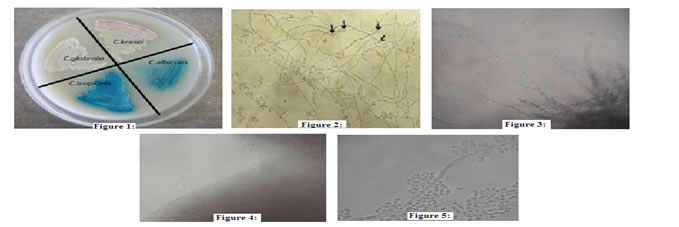
Figure 1: CHROM agar showing different coloured growth of Candida species; Figure 2: Chlamydospores of Candida albicans seen on corn meal agar; Figure 3: Candida tropicalis showing blastospores singly or in very small groups all along the pseudohyphae in cornmeal agar; Figure 4: Candida glabrata showing small spherical, highly compacted yeast cells without pseudohyphae on corn meal agar; Figure 5: Candida krusei showing pseudomycelia with elongated blastospores forming “tree-like” appearance
DISCUSSION
In spite of several treatment modalities and application of new effective drugs, VVC is a complex and considerable problem in gynecology and obstetrics.3 On the other hand, different studies in different countries have illustrated that the Candida species involved in this disease along with their susceptibility to antifungal agents, is also changing in recent years.4-7 In the present study, the most common Candida species isolated was Candida albicans which accounted for 22/42 (52.4%) of total Candida species isolated whereas Non-albicans Candida(NAC) accounted for the rest 20/42 (47.6%) of the growth. Among NACs most common species isolated was Candida tropicalis15/42 (35.7%) followed by Candida krusei 3/42 (7.1%). The least isolated species was Candida glabrata accounting for 2/42(4.8%) of total growth. In the study reported from Amritsar by Jindal et al,8 C.albicans was the most common isolate(69.57%)which is similar to the present study. Among 30.43% of NACs in this study, the most common species was C.glabrata (8.7%) while C.tropicalis predominated in the present study. In Vijaya et al study9 conducted in Karnataka, C.albicans was the most common species isolated 35/53 (66%) followed by NACs 18/53 (34%).Among NACs commonest species was C.tropicalis (26.4%) followed by C.krusei (3.8%) and the least was C.glabrata(1.9%). This study was consistent with the present study. In the study conducted by Vijaya et al9 and also in the present study, C.tropicalis was the most common NAC species isolated unlike in other studies where C.glabrata or C.krusei was the major isolate.10-12 On comparison of various studies, it was observed that in most of the studies, including the present study, C.albicans was the predominant species isolated.C.albicans adheres to vaginal epithelial cells in significantly higher numbers than other Candida species which could be the reason for the relative infrequency of the latter in vaginal candidiasis.12 In contrary to the present study, the study conducted by Kalaiarasan et al,13 showed non albicans candida as the predominant species causing VVC. Kalaiarasan et al reported C.glabrata (45.1%) as the most common isolate followed by C.tropicalis (23.5%), C.albicans (17.6%) and C.krusei (9.8%). Various other studies have also reported C.glabrata as the most common pathogen isolated from VVC.14-16 An increase in the prevalence of NAC vaginitis is seen in many studies.12,17-20 The possible reason for this may be the increased indiscriminate usage of antimycotics which removes the more sensitive C.albicans and selects more azole‐resistant NAC species.17,20
CONCLUSION
Candida albicans predominated in this study followed by C. tropicalis, C. krusei and C. glabrata. Presumptive identification followed by confirmation of yeast species helps in initiating an early and appropriate antifungal therapy thereby reducing the morbidity.
REFERENCES
1. Emerib AU, Nasir IA, Onyia J, Ifunanya AL. Prevalence of vulvovaginal candidiasis among non-pregnant women attending a tertiary health care facility in Abuja, Nigeria. Research and Reports in Tropical Medicine 2015; 6: 37-42.
2. Chander J. Textbook of Medical Mycology. 3rd ed; 2009. Mehta pub.pp.266.
3. Graeme Dennerstein Review. The treatment of candida vaginitis and vulvitis. JAMA India 2001; 4: 50-2.
4. Anderson MR, Klink K, Cohrssen A. Evaluation of vaginal complaints. JAMA. 2004; 291:1368-79.
5. Trama JP, Adelson ME, Raphaelli I, Stemmer SM, Mordechai E. Detection of Candida species in vaginal samples in a clinical labora¬tory setting. Infect Dis Obstet Gynecol. 2005; 13(2):63–7.
6. Jamilian M, Mashadi E, Sarmadi F, Banijamali M, Farhadi E, Ghanatpishe E. Frequency of vulvovaginal Candidiasis species in non¬pregnant 15-50 years old women in spring 2005 in Arak. Arak Univ Med Sci J. 2005; 10(2):7–14.
7. Etminan S, Zarinkatsh H, Lotfee M. The Prevalence of Candida Vaginitis among Women aged 15-49 Years in Yazd, Iran. Med Lab J. 2008; 2(1):39-45.
8. Jindal N, Aggarwal A, Gill P. Significance of candida culture in women with vulvovaginal symptoms; J ObstetGynecol India 2006;56(2):139-141.
9. Vijaya D, Dhanalakshmi TA, Kulkarni S. Changing trends of vulvovaginal candidiasis. J Lab Physicians. 2014 Jan; 6(1):28-30.
10. Rosa MI, Silva BR, Pires PS, Silva FR, Silva NC, Silva FR, Souza SL, Madeira K, Panatto AP, Medeiros LR: Weekly fluconazole therapy for recurrent vulvovaginal candidiasis: a systematic review and meta-analysis. Eur J ObstetGynecolReprodBiol2013; 167: 132–136.
11. Abdelmonem AM, Rasheed SM, Mohamed AS. Bee-honey and yogurt: a novel mixture for treating patients with vulvovaginal candidiasis during pregnancy. Arch GynecolObstet2012; 386: 109–114.
12. Omar AA. Gram stain versus culture in the diagnosis of vulvovaginal Candidiasis. East Mediterr Health J 2001; 7: 925‐34.
13. Kalaiarasan K, Singh R, Chaturvedula L. Fungal Profile of Vulvovaginal Candidiasis in a Tertiary Care Hospital. J Clin Diagn Res. 2017 Mar;11(3).
14. Mohanty S, Xess I, Hasan F, Kapil A, Mittal S, Tolosa JE. Prevalence and
susceptibility to fluconazole of Candida species causing vulvovaginitis. Ind J
Med Res. 2007; 126(3):216-19.
15. Kumar CPG, Menon T. Biofilm production by clinical isolates of Candida species. Med Mycol. 2006; 44(1):99-101.
16. Ray D, Goswami R, Banerjee U, Dadhwal V, Goswami D, Mandal P, et al.
Prevalence of Candida glabrata and its response to boric acid vaginal suppositories in comparison with oral fluconazole in patients with diabetes and vulvovaginal candidiasis. Diabetes Care. 2007; 30(2):312-17.
17. Nabhan A. Vulvovaginal candidiasis. Ain Shams J ObstetGynecol2006; 3: 738.
18. Sobel JD, Faro S, Force W et al. Vulvovaginal candidiasis; epidemiologic,
diagnostic and therapeutic consideration. Am J Obstet and Gynecol1998; 178: 203-11.
19. Kent HL. Epidemiology of vaginitis. Am J ObstetGynecol1991; 165: 1168-76.
20. Ambiye VR, Shahani S, Pawar D. Role of fluconazole in vaginal candidiasis. The Indian Practioner2000; 53: 805-8.
 Home
Home This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.