 Home
Home
|
Table of Content Volume 13 Issue 3- March 2020
Study of oculomycosis in a tertiary care CENTRE-VIMS Ballari
Thipperudraswamy T1, Shilpa H S2*
1Associate Professor, Department of Microbiology, BLCMCRI, Bangalore, Karnataka, INDIA. 2Assisstant Professor, Department of Microbiology, Siddartha Medical College Tumkur. Email: trsganeshjai@gmail.com
Abstract Background: Oculomycosis is common in both tropical and subtropical areas and is caused by all types of fungi. The commonest predisposing factor is trauma. Objective: To find out the prevalence of oculomycosis in patients with corneal ulcer. Materials and Methods: A total of 332 samples from corneal ulcer were received from January 2015 to December 2015. The affected eye was cleaned with sterile normal saline and anaesthetized .With Bard Parker Blade Corneal scrapping no .15 the entire base of ulcer as well as the edges were thoroughly scraped .Corneal scraping was subjected to 10% KOH mount and Gram staining and cultured on Sabouraud dextrose agar with and without antibiotics. Fungal growth was identified by standard mycological technique. Results: Out of 332 samples collected, 66 (19.87%) revealed hyphae in direct KOH mount and 50(15.06%) showed fungal culture positive .Among the fungal isolates ,Aspergillus niger (36%) was more prevalent followed by Aspergillus flavus(22%) and Fusarium spp(12%), Candida spp(8%), Penicillium spp(6%), Alternaria spp(6%), Bipolaris spp(6%), and Mucor spp(4%),Rhizopus(4%), Exserohilum(2%) and Paecilomyces spp(2%). Conclusion: Aspergillus niger is the commonest cause of oculomycosis .This study also emphasized the need of performing both a direct KOH mount examination and culture to improve sensitivity . So proper understanding of agent and host factors involved in infection will improve the outcome of the condition. Key Words: Oculomycosis, Aspergllus.
INTRODUCTION The cornea is the transparent avascular anterior most structure of the eye measuring 10-12mm in diameter . It has a central thickness of about 0.5mm .It is ocular structure most frequently damaged by external trauma1.Fungal keratitis was first described by Leber in 1879(Centers for Disease Control and Prevention ,2013;Singh,2011) 2. The etiological and epidemiological features of infective keratitis depend on host factors, geographical location and climate. Several risk factors like age , sex , immune status and socioeconomic background determine the pathogenesis of infective keratitis3. Fungi cannot penetrate the intact corneal epithelium and do not enter the cornea from episcleral linear vessels. The principal routes of inoculation are introduction concurrent with a penetrating or perforating wound either mechanical injury or surgery and introduction through an epithelial defect 2. Invasiveness of corneal tissue may be aided by formation of intrahyphal hypae or by alterations in fungal morphology such as thickening of the fungal cell wall. Liberation of fungal proteinases or toxins and polymorphonuclear leucocytes , augment fungal invasion resulting in extensive degradation of corneal tissue matrix coagulation necrosis associated with loss of keratinocytes and edematous changes of collagen fibers occur. Satellite lesions are formed late in course of the disease process, hypopyon occurs with hyphae encased in dense neutrophilic exudates encased in dense neutrophilic exudates leucocytic infiltrate with feathery borders in corneal stroma is characteristic of fungal keratitis 6.
The prospective study was done in VIMS Ballari in patients presenting with suspected microbial keratitis attending ophthalmology department7. A total of 332 samples from corneal ulcer were received from January 2015 to December 2015. A detailed history was noted . History of trauma to the eye was specifically taken. The affected eye was cleaned with sterile normal saline and anaesthetized using 4% xylocaine drops .With Bard Parker Blade Corneal scrapping no .15 the entire base of ulcer as well as the edges were thoroughly scraped. Material collected in one scraping is used to inoculate culture plates material collected in an additional scraping is used to prepare smears or mounts for direct microscopic examination5. Corneal scraping was subjected to 10% KOH mount and Gram staining and cultured on culture plates in the form of multiple ‘C’s; only growth on the ‘C’-streaks was deemed significant. Material was inoculated in Sabouraud dextrose agar with and without chlramphenicol. Fungal growth was identified by standard mycological technique5. In the microbiology laboratory SDA tubes were incubated both at room temperature and at 37 oc for up to a maximum of one month. Cultures not showing fungal growth within a month were considered to be negative . Identification of the fungus was done by taking some of the growth from the Sabouraud’s dextrose agar slant and mounting it on a slide. It was stained with Lacto phenol cotton blue and examined under the microscope5.
RESULTS A total of 332 corneal scrapings were collected from 332 patients presenting with suspected microbial keratitis attending ophthalmology department VIMS ,BALLARI.
Table 1: Demographical analysis:
Among 332 patients 192(57.8%) were males and 140(42.2%) were females.
Table 2: AGE INCIDENCE
The above table shows among 332 patients , majority of the patients were from 41-50 years (44.8%) age group followed by the age group 61-70 (20.48%) in both the genders. Least number were from 11-20 (1.2%) age group patients.
Table 3: AGE AND SEX WISE DISTRIBUTION OF KOH POSITIVE PATIENTS
Out of 332 patients 66 (19.87%) revealed hyphae in direct KOH mount .Among them 36 were males and 30 were females. Majority of the KOH positive patients were between age group 41-50 24(36%) which included 13 males and 11 females .Least number of KOH positive patients were from age group21-30(4.5%) included 2 males and single female.
Table 4: AGE AND SEX WISE DISTRIBUTION OF FUNGAL CULTURE POSITIVE PATIENTS
Above table shows that 50(15%) patients were culture positive among 332 patients presented with microbial keratits .Among these culture positive patients 30 (60%)were males and 20 (40%)were females .Majority of the culture positive patients were between 41-50 22 (44%)age group in both genders which included 13 males and 9 females. Culture remained sterile between age group 11-20.
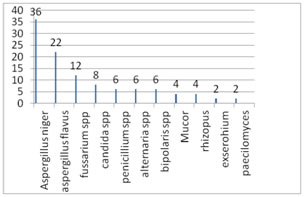
Graph 1: ETIOLOGICAL AGENTS GROWN ON CULTURE
Among the fungal isolates ,Aspergillus niger (36%) was more prevalent followed by Aspergillus flavus(22%) and Fusarium spp(12%), Candida spp(8%), Penicillium spp(6%), Alternaria spp(6%), Bipolaris spp(6%), and Mucor spp(4%),Rhizopus(4%), Exserohilum(2%) and Paecilomyces spp(2%). DISCUSSION A variety of factors determine clinical outcome in microbial keratitis and the epidemiological patterns vary from one country to the other and in geographical areas in the same country .A comprehensive data is important to develop appropriate diagnostic and therapeutic strategies5. This study reports 332 samples 60(19.87%) were found to be positive for fungal elements by direct KOH mounts. In other studies conducted by Rubeena et al , J M Jacob et al 60%, 39.4% were found to be positive by direct microscopy with KOH mount. In present study maximum number of cases were observed between age group 51-60years i.e. elderly patients which correlated with the finding Vijay S Rajmane et al 6. Maximum number of cases was recorded in months of October to February (60%) which corresponded with harvesting season of this part of country. Similar finding reported by Kotigadde et al9. The male preponderance in this series was not only in the overall clinically suspected cases of microbial keratitis but also culture – proven cases of microbial keratitis5. In our study Aspergillus niger is major etiological agent of oculomycosis which is similar to study conducted by Vijay S Rajmane et al 6,Kotigadde et al 11 and Sharma et al 9. In present study followed by Aspergillus niger and Aspergillus flavus ,Fusarium was third most predominate fungal isolate which also correlates with study done by Vijay S Rajmane et al6. But in study conducted by Bharathi et al12 and Srinivasan et al 10Fusarium was predominate agent causing oculomycosis. Among rare fungi causing oculomycosis 3 Alternaria spp, Bipolaris spp ,Penicillium spp was isolated followed by single isolate of paecilomyces spp and Exserohilum were isolated in present study . Similar rare fungi are isolated from earlier studies done by Bharathi et al 12. PHOTOGRAPH OF KOH MOUNT GRAM
GRAM STAIN
LPCB MOUNT
CONCLUSION Aspergillus niger is the commonest cause of oculomycosis .This study also emphasized the need of performing both a direct KOH mount examination and culture to improve sensitivity. So proper understanding of agent and host factors involved in infection will improve the outcome of the condition.
REFERENCES
Policy for Articles with Open Access
|
|

 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.