 Home
Home
|
Table of Content Volume 14 Issue 1 - April 2020
Bacterial profile and antimicrobial susceptibility patterns of otitis media in health care centre, southern Trivandrum, Kerala, India
Jobin S R1*, J W Prakash2, Jagatheeswary P A T3, Rema Devi S4, Subitha S5, L Suresh Babu6, Kiran Gopal7, Bewin Oral J8, P S Aanie9
1Assistant Professor, 4,6,7,8 Department of Microbiology, Dr. Somervell Memorial C.S.I. Medical College, Karakonam, Trivandrum, Kerala, INDIA 695504. 2Adjunct Associate Professor, Martin Luther Christian University, Shillong, INDIA. and Hon. Associate Scientist, Environmental Resource Research Centre, Mahatma Gandhi University, Kerala & Project Co Ordinator Dr. Somervell Memorial C.S.I. Medical College, Karakonam, Trivandrum, Kerala, INDIA. 3Professor, Department of Microbiology, Saveetha Medical College, Saveetha University, Chennai, Tamil Nadu, INDIA. 5,9Research Scholar, Manonmaniam Sundaranar University, Tirunelveli, Tamil Nadu, INDIA. Email: jobinsr2017@gmail.com
Abstract Background: Ear infection is a common problem for both children and adults particularly in developing countries. Thus this study aimed to identify bacterial isolates and determine their drug susceptibility pattern from patients who had ear infection. Cross sectional study was carried out on patients with ear infection from January 2019 to September 2019.For this study 37 samples were collected from patients in the rural area of Trivandrum, Kerala. In this study, pathogens were isolated from 29 (78.37%) patients out of 37.Staphylococcus aureus 5 (17.24 %), Proteus mirabilis 2 (6.89 %), Pseudomonas aeruginosa 15 (51.72 %) Klebsiella pneumoniae 6 (20.68%) and Escherichia coli 1 (3.44%) were the bacterial isolate respectively. The Gram negative bacteria were more dominant than Gram positive. The Staphylococcus aureus isolated were resistant to Penicillin (100 %) Erythromycin (80 %) Clindamycin (60%), Amoxicillin clavulanic acid (60%) and Gentamicin (20 %). The Pseudomonas aeruginosa were resistant to Aminoglycosides (13.33 %). The organism Proteus mirabilis shows 100% sensitivity towards Amoxicillin clavulanic acid, Gentamicin, Amikacin, Cefazolin, Cefuroxime, Cefotaxime, Ciprofloxacin, Co-trimoxazole, Piperacillintazobactum, Cefaperazonesulbactum. Escherichia coli isolates showed 100% resistance to Ampicillin, Amoxicillin clavulanic acid, Cefazolin and Cefuroxime. Klebsiella pneumoniae isolates have shown resistance to Amoxicillin clavulanic acid (16.66 %), Gentamicin (33.33 %), Amikacin (33.33 %), Cefazolin (33.33 %), Cefuroxime (33.33 %), Cefotaxime (33.33 %) and Piperacillintazobactum (16.66 %). Early treatment of ear infection can play great role in management of otitis media and avoid emergence of multi drug-resistant bacteria. Key words: Bacteria, Otitis Media, Antimicrobial Susceptibility.
INTRODUCTION Ear infection is a common clinical problem throughout the world and the major cause of preventable hearing loss in the developing world (Ullauri et al., 2014). Ear infection which can be classified into Otitis Media (OM) and Otitis Externa, is a major public health concern in developing countries. (Monasta et al.., 2012)Otitis media (OM) is a general term for the expression of infections with various complications in the middle‑ear region. OM is divided into three categories: acute OM, OM with effusion, and Chronic Suppurative OM (CSOM) (Gates et al., 2002). The CSOM condition occurs as asequelae to inadequately treated acute otitis media causing persistent perforation in the tympanic membrane which could be infected from bacteria in the external auditory canal (Jyothi et al.., 2017).Globally, about 65-330 million people suffer from ear infection and 60 % of them had significant hearing impairment (Woodfield and Dugdale, 2008).The causative agents of ear infection might be bacterial, viral, or fungal. However, the major causative agents of ear infection are bacterial isolates such as Pseudomonas aeruginosa, Escherichia coli, Staphylococcus aureus, Streptococcus pyogenes, Proteus mirabilis, Klebsiella spp., or mixed bacterial infection (Afolabi et al.., 2012). Development and spread of resistant bacteria due to the over and indiscriminate use of antibiotics was a global public health threat.(Spellberg et al..,2008).Due to the limited laboratory diagnosis in developing countries, physicians are often forced to syndromatic diagnosis and prescription of broad spectrum antibiotics for most infections that led to emergence of drug resistant bacterial strains (Lee et al.. 2012). Hence, current information on microbial resistance and the prevalence of the pathogenic bacteria needs to be available at national and local levels to guide the rational use of the existing antimicrobials. In Kerala, few studies reported high prevalence of ear infection and multi drug resistance to the commonly prescribed antibiotics for treatment of ear infection (Muluye et al. 2013) However, there is no published data from study area on the prevalence and antimicrobial susceptibility pattern of bacterial pathogens causing Otitis Media. Hence, current information on prevalence of pathogenic bacteria and their susceptibility pattern must be available at national and local levels to guide the rational use of the existing antimicrobials.
METHODOLOGY A cross-sectional study was conducted at health care center Trivandrum, Kerala. Patients who visited the ENT clinic of the hospital with otitis media from January 2019 to September 2019 were consecutively enrolled into the study. A total of 37 ear discharges samples were collected by Otorhinolaryngologist using sterile cotton swabs. Specimens were inoculated directly on Blood agar, Chocolate agar and MacConkey agar following the standard procedure of inoculating culture media. Isolates were identified by colony morphology, Gram staining, Catalase test, Coagulase test, Oxidase test, Triple Sugar Iron agar (TSI), Citrate utilization test, Urease test, Mannitol Motility, Indole and Optochin test (Cheesbrough 2006). Antimicrobial sensitivity test (AST) was done on Mueller Hinton agar (Microxpress, A Division of Tulip Diagnostics (P) Ltd.India) by the Kirby-Bauer technique according to the CLSI guidelines (CLSI-2007) using Escherichia coli (ATCC 25922), Staphylococcus aureus (ATCC 25923) and Pseudomonas aeruginosa (ATCC 27853) as control strains. The antibiotic discs used for the AST included: Ampicillin (10mcg), Cefazolin (30mcg), Amikacin (30 mcg), Amoxycillin/clavulanic acid (20/10 mcg), Cefotaxime (30mcg), Cefuroxime (30 mcg), Ceftazidime (30mcg), PiperacillinTazobactum ( 100/10mcg) , Gentamicin (10mcg), Cephoperazone + sulbactam (75/10 mcg), Cotrimoxazole (1.25/23.75mcg), Ciprofloxacin (5 mcg), Linezolid (30 mcg), Meropenem (10 mcg), Norfloxacin (10 mcg), Cloxacillin (1 mcg), Tobramycin (10 mcg) Netilmicin, Tetracycline and Vancomycin (30 mcg) from Microxpress, A Division of Tulip Diagnostics (P) Ltd. India.
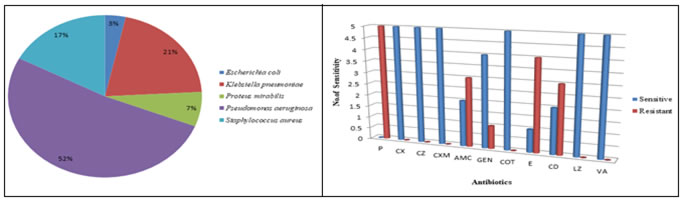
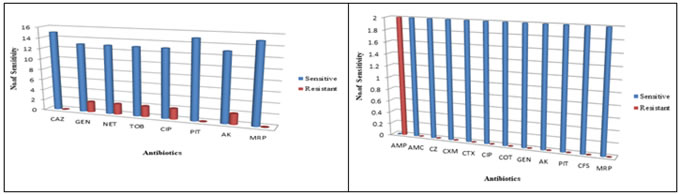
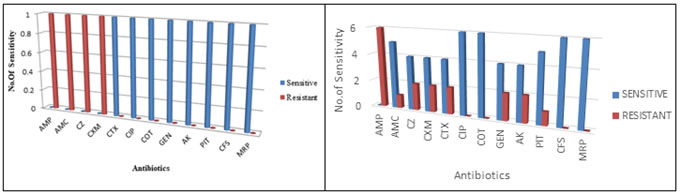
RESULTS The age range of participants for this study was from all age groups. For this analysis 37 samples were collected. They were from the rural areas of Trivandrum, Kerala. In this study, pathogens were isolated from 29 (78.37%) patients out of 37. The study was conducted among both males and females. Among the total number of patients 18 (62.06%) were males and 11 (37.93%) were females (Table1.). The highest percentage of isolates were reported in below 10 years (62.06%) and followed by 71-80 (20.68%) (Table. 2.). The highest number of patients were reported during February 5 (17.24%) and followed by May and July 4 (13.79) (Table. 3.).Staphylococcus aureus 5 (17.24%), Proteus mirabilis 2 (6.89 %), Pseudomonas aeruginosa 15 (51.72%) Klebsiella pneumoniae 6 (20.68 %) and Escherichia coli 1 (3.44%) were the bacterial isolates respectively (Fig.1). The Gram negative bacteria 24 (82.75%) were more predominant than Gram positive 5 (17.24 %). In vitro antibiotic susceptibility of Gram positive bacterial isolates were experimented. From the isolates Staphylococcus aureus was the only one reported as Gram positive bacteria and were resistant to Penicillin (100 %) Erythromycin (80 %) Clindamycin (60%), Amoxicillin clavulanic acid (60%) and Gentamicin (20 %).The isolates were all sensitive to Cloxacillin, Cefazolin, Cefuroxime, Co-trimoxazole, Linezolid and Vancomycin shown 100% sensitivity (Fig.2).The Pseudomonas aeruginosa was resistant to Aminoglycosides (13.33 %). The Fluoroquinolone Ciprofloxacin shows 13.33% resistance. Ceftazidime, Piperacillintazobactum and Meropenem showed 100 % sensitivity (Fig.3).The organism Proteus mirabilis shows 100% sensitivity towards Amoxicillin clavulanic acid, gentamicin, Amikacin, Cefazolin, Cefuroxime, Cefotaxime, Ciprofloxacin, Co-trimoxazole, Piperacillintazobactum, Cefaperazonesulbactum and Meropenem (Fig.4). Escherichia coli showed 100% resistance to Ampicillin, Amoxicillin clavulanic acid, Cefazolin, and Cefuroxime. Whereas, Cefotaxime, Gentamicin, Amikacin, Ciprofloxacin, Co-trimoxazole, Piperacillintazobactum, Cefaperazonesulbactum and Meropenum were 100% sensitive (Fig.5). Klebsiella pneumonia have shown resistance to Amoxicillin clavulanic acid (16.66 %), Gentamicin (33.33 %), Amikacin (33.33 %), Cefazolin (33.33 %), Cefuroxime (33.33 %), Cefotaxime (33.33 %) and Piperacillin tazobactum (16.66 %) (Fig.6).
Figure 1: Pathogens isolated from otitis media patients Figure 2: Antibiogram of Staphylococcus aureus P- Penicillin, CX- Cloxacillin, CZ-Cefazolin, CXM-Cefuroxime, AMC-Amoxycillin/clavulanic acid,GEN-Gentamicin, COT-Cotrimoxazole,E-Erythromycin,CD-Clindamycin,LZ-Linezolid,VA-Vancomycin
Figure 3: Antibiogram of Pseudomonas aeruginosa Figure 4: Antibiogram of Proteus mirabilis CAZ- Ceftazidime, GEN- Gentamicin, NET- Netilmicin, TOB- Tobramycin, CIP- Ciprofloxacin, PIT- PiperacillinTazobactum, AK- Amikacin, MRP- Meropenem AMP-Ampicillin, AMC- Amoxycillin/clavulanic acid, CZ- Cefazolin, CXM- Cefuroxime, CTX- Cefotaxime, CIP-Ciprofloxacin,COT- Cotrimoxazole, GEN- Gentamicin, AK-Amikacin, PIT- PiperacillinTazobactum, CFS- Cephoperazone + sulbactam, MRP- Meropenem
Figure 5: Antibiogram of Escherichia coli Figure 6: Antibiogram of Klebsiella pneumoniae AMP- Ampicillin, AMC- Amoxycillin/clavulanic acid, CZ- Cefazolin, CXM- Cefuroxime, CTX- Cefotaxime, CIP-Ciprofloxacin, COT- Cotrimoxazole, GEN- Gentamicin, AK-Amikacin, PIT- PiperacillinTazobactum, CFS- Cephoperazone + sulbactam, MRP- MeropenemTable 1: Sex Vs Isolation (%)
Table 2: Age Distribution
Table 3: Monthly Distribution
DISCUSSION In this study the prevalence of bacteria among otitis media patients in the health care centre was 78.37 %. This finding coincides with the findings of Seid et al. 2013 and Muluye et al. 2013. The present study shows that males are more commonly affected than females. Male predominance may be because of their more exposed way of life. The report of Kiran et.al., 2019 is same that of this study. Less than 10-year-old patients were significantly colonized by bacterial pathogen and this result is coinciding with the findings of Iseh and Adegbite 2004. Low immune status, shorter and horizontal nature of their Eustachian tubes, frequent exposure to upper respiratory tract infections and malnutrition could be the possible justifications for the high infection in this age group. The monthly reports of Otitis media was most common in February (17.24%) and this findings are similar to the study done by Kiran et.al., 2019. The Gram-negative bacteria, 82.75 % were the dominant isolates of the samples compared to Gram- positive bacteria. Parallel reports were seen in the research documents of Abera and Kibret 2011 and Ferede et al. 2001). The bacteria Staphylococcus aureus, Proteus mirabilis and Pseudomonas aeruginosa, Klebsiella pneumoniae and Escherichia coli were the overriding isolates in this study. This was in line with finding from Addis Ababa (Ferede et al. 2001). Pseudomonas aeruginosa, was the dominant cause of OM in this study was reported as same that of Weckwerth et al. 2009. The disparity in climatic and geographic could be the probable reasons for the distinction in distribution of the bacteria. In this study monoclonal infection was seen in 100 % of the patients. This observation was supported by other researchers like Ettehad et al. 2006. In contrast to this, other study from India is reported (Kumar and Seth 2011). The Prevalence of coliforms bacteria such as Proteus mirabilis, Klebsiella pneumonia and Escherichia coli in this study was tandem to reports by Prakash et al. 2013, Mansoor et al. 2009 and Shyamala and Reddy (2012). In vitro antimicrobial susceptibility pattern revealed that isolates were highly resistant to most antibiotics. Staphylococcus aureus were 100 % resistant to Penicillin. This result was in line with that of study done Osazuwa et al. 2011and Prakash et al. 2013. However Staphylococcus aureus isolates were less resistant for gentamicin, which was similar with the results of other researches Abera and Kibret 2011. Pseudomonas aeruginosa was sensitive to ciprofloxacin and this result is as same that of the findings of Yismaw et al. 2010 and Rao and Bhaskaran 1984”. All isolates of P. mirabilis were 100 % sensitive to ciprofloxacin and this was in concurrence with Prakash et al. 2013.
CONCLUSION Most of the isolates showed resistance to antimicrobial agents. However, bacterial isolates were sensitive to ciprofloxacin and gentamicin. This can be used in the treatment of otitis media. Early treatment of ear infection can play great role in management of otitis media and avoid further emergence of multi drug-resistant bacteria. Acknowledgement The authors gratefully acknowledge the tremendous support and encouragement of Dr. J. Bennet Abraham (Director, Dr.S.M.C.S.I.M.C.and H.), Dr.SamsonNessaiah (Principal, Dr.S.M.C.S.I.M.C.and H.) and all other well-wishers for the successful completion of this research work.
REFERENCE
Policy for Articles with Open Access
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.