 Home
Home
|
Table of Content Volume 14 Issue 2 - May 2020
L Suresh Babu1*, S R Jobin2
1Professor, 2Assistant Professor, Department of Microbiology, Dr Somervell Memorial CSI Medical College & Hospital, Karakonam, Trivandrum District, Kerala, Pincode- 695504, INDIA. Email: sureshbabu6831@yahoo.in
Abstract Background: Urinary tract infection is the second most common community acquired infection next to respiratory infections. There are few reports of UTI elsewhere in India, but, it is very little in Kerala, that too in the rural areas of Trivandrum district, there is no report covering the antibiotic resistance pattern of the common UTI isolates. So, we have undertaken this study, so as to understand the ever increasing antibiotic resistance pattern of common UTI pathogens in this part of the country. Urine samples were collected between a period of 1-1-2018 and 13-2 2018. Out of the 1000 samples collected during this period, we have isolated 168(16.8%) pathogens, predominantly bacterial and few fungal agents, from the corresponding 168 UTI cases. Out of these 168 UTI cases, 40 (23.8%) were male and 128 (76.2%) were female. Outpatients (54.8%) predominated over the inpatients (45.2%). Among the uropathogens isolated, Escherichia coli was the dominant (69.6%) organism followed by Klebsiella spp. (9.5%), with very few isolates of Enterococcus spp., Staphylococcus aureus, Candida spp., Acinetobacter spp, Pseudomonas spp., Proteus mirabilis and Citrobacter spp, in that order. E. coli being the most predominant isolate, showed increased resistance to Amoxiclav(85.5% of isolates), followed by Nalidixic acid (75.3%), Amoxicillin (73.5%,), Cefuroxime (54.7%), Cefixime (53.8%), Cefotaxime (52.2%), Ciprofloxacin (46.2%) and Norfloxacin (40.2%). Similarly, Klebsiella spp., the second most isolates, reported higher level of resistance to Amoxiclav (87.5% of isolates), followed by Amoxicillin (56.3%), Cefuroxime (43.7%), Cefixime (37.5%) and Co-trimoxazole (37.5%). Among the few isolates of Enterococcus spp., the strains exhibited maximum resistance to Norfloxacin (75% of strains) followed by Penicillin (41.7%). In Staphylococcus aureus isolates, 50% of them showed resistance to Penicillin, but no MRSA recorded. Seven multi-drug resistant strains, 4 of E. coli, 2 of Klebsiella spp. and one of Acinetobacter sp., were also seen. Key words: E. coli, Enterococcus spp., Klebsiella spp., Multi-drug resistant, Trivandrum district, UTI.
INTRODUCTION Urinary tract infections (UTIs) are one of the commonly encountered diseases in developing countries with an estimated annual global incidence of at least 250 million.1 Although UTIs occur in both men and women, clinical studies suggest that the overall prevalence of UTI is higher in women. Uncomplicated UTIs in healthy women have an incidence of 50 individuals among 1000 women in a year.2 Almost 95 % of cases of UTIs are caused by bacteria.3 Up to 85% of UTIs are caused by Escherichia coli.4 Excessive and/or inappropriate use of antibiotics in treating UTIs is responsible for the emergence and spread of multi-drug resistant (MDR) urinary bacteria 5. There are three mechanisms that can cause antibiotic resistance. Prevention of the interaction of the drug with target organisms, decreased uptake due to either an increased efflux or a decreased influx of the antimicrobial agent, and enzymatic modification or destruction of the compound 6. There were few reports of the resistance rate of uropathogenic E. coli to various antibiotics are available elsewhere in India.7,8,9,10 But, the resistance pattern of community acquired uropathogens has not been extensively studied in the Indian subcontinent.11,12,13 There was one report of antibiotic susceptibility pattern of uropathogens recorded in north Kerala 14, but, none were so far available in South Kerala, that too in rural areas of this region. By keeping all these in mind, we have undertaken this work to study in detail the ever increasing trend in the resistance of uropathogens against common antibiotics, in the rural areas of southern part of Trivandrum district, Kerala.
MATERIALS AND METHODS The work has been carried out in the department of Microbiology, Dr Somervell Memorial CSI Medical College and Hospital, Karakonam, Trivandrum district, Kerala, India. A total of 1000 midstream urine samples from suspected cases of urinary tract infections were collected in pre-sterilized disposable universal containers, during a period between 1-1-2018 and 13-2-2018 at the microbiology diagnostic laboratory, Dr SM CSI Medical College and Hospital. The samples were processed within 1hr of collection as per the standard procedures. A wet mount with the deposit was done first to look for pus cells and/or bacteria, followed culture on to 5% sheep blood agar and MacConkey agar, purchased from HiMedia, Mumbai, by the standard semi-quantitative calibration loop technique making use of 0.001 ml diameter loop. The plates were incubated at 37oC overnight and looked for growth. Those samples yielded 100 colonies or more (105 CFU/ml of urine) in both the media were considered as showing significant bacteriuria for ascertaining definite UTI.15,16 Out of the total 1000 urine samples processed, 168 (16.8%) showed significant bacteriuria and hence were considered as definite UTI cases. Of these 168 UTI cases, 92 (54.8%) were from OPDs, 45 (26.8%) from peripheral multi-speciality hospitals and remaining cases were from intensive care units and other medical wards (Table-5). The organisms isolated from these cases were identified by their colony and biochemical characteristics. 117 (69.4%) of the isolates were Escherichia coli, 16 (9.5%) belonged to Klebsiella spp., followed by Enterococcus spp., 12 (7.1%), Staphylococcus aureus, 6 (3.5%), Candida spp., 5 (2.9%), Acinetobacter spp., 4 (2.4%), 3 (1.8%) each of Pseudomonas spp and Proteus mirabilis and 2 (1.2%) of Citrobacter spp., (Table-6). All the 168 isolates were subjected to antibiotic susceptibility testing by Kirby- Bauer disc diffusion method in Mueller- Hinton agar, except, Enterococcus isolates, for which it was done in 5% sheep blood agar, based on the CLSI guidelines. ATCC strains one each of the isolates of bacterial pathogens were employed as quality control.17 The antibiotic discs used were, Ampicillin (10 mcg), Amikacin (30 mcg), Amoxicillin+Clavulanic acid (30 mcg), Chloramphenicol (30 mcg), Ciprofloxacin (5 mcg), Cloxacillin (200 mcg), Co-trimoxazole (25 mcg), Cephotaxime (30 mcg), Cefuroxime (30 mcg), Cefaclor (30 mcg), Cefixime (30 mcg), Cefazolin (30 mcg), Gentamicin (10 mcg), Linezolid (10 mcg), Meropenem (10 mcg), Nofloxacin (10 mcg), Nalidixic acid (30 mcg), Penicillin (10 units), Piperacillin+ Tazobactam (100/10 mcg), Rifampicin (5 mcg), Tobramycin (10 mcg) and Vancomycin (30 mcg), procured from HiMedia, Mumbai. The plates were incubated at 37oC overnight for every isolate then and there, and the zone inhibition was measured in millimetres to ascertain, whether a particular antibiotic is sensitive or resistant to an isolate, by interpreting from the chart supplied by the disc manufacturer (HiMedia, Mumbai).
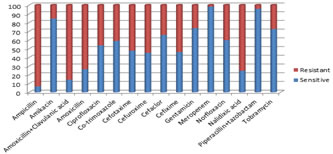
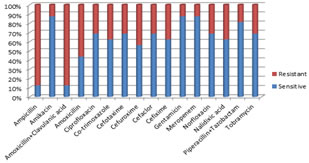
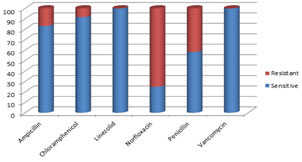
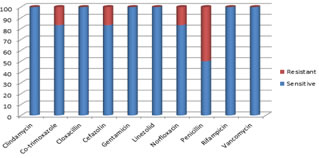
OBSERVATIONS AND RESULTS Out of the 168 UTI cases, 40 (23.8%) were male and 128 (76.2%) were female [Table-1]. The age group of 31-40 and 61-70 showed the highest distribution of cases of 29 (17.2%) each, followed by 21-30 of 27 (16%), 51-60 and >70 groups had 23 (13.6%) cases each [Table-2]. Among male, >70 age group were the most infected UTI cases, of 13 (32.5%), [Table-3] and in female, 21-30 age group had the highest UTI cases of 27 (21%), followed by 31-40 having 23 (17.9%) cases, [Table-4]. Out patients, out numbered the in-patients among the UTI cases, having 92 (54.8%), followed by peripheral health care centres, 45 (26.8%), female medical ward, 15 (8.9%) and few cases distributed among intensive health care units [Table-5]. Out of the total 168 confirmed UTI cases, Escherichia coli was the most predominant isolate from 117 (69.6%) cases, followed by Klebsiella spp., 16 (9.5%), Enterococcus spp., 12 (7.1%), Staphylococcus aureus, 6 (3.5%), Candida spp., 5 (2.9%), Acinetobacter spp., 4 (2.4%), Pseudomonas spp., and Proteus mirabilis 3 (1.8%) each and Citrobacter spp., 2 (1.2%), [Table-6]. Escherichia coli being the predominant isolate, showed the highest level of resistance to Ampicillin (93.2%), followed by Amoxiclav (85.5%), Nalidixic acid (75.3%), Amoxicillin (73.5%), Cefuroxime (54.7%), Cefixime (53.8%), Cefotaxime (52.2%), Ciprofloxacin (46.2%) and Norfloxacin (40.2%). Meropenem remained the most sensitive drug (98.3%), followed by Piperacillin+Tazobactam (95.7%), Amikacin (84.7%), Gentamicin (73.5%) and Tobramycin (72.6%), [Table-7, Figure-1]. Among Klebsiella spp., Ampicillin and Amoxiclav were the most resistant antibiotics (87.5%), followed by Amoxicillin (56.3%), Cefuroxime (43.7%) and Cefixime and Co-trimoxazole, 37.5% each. Meropenem, Gentamicin and Amikacin were the most sensitive drugs (87.5%), followed by Piperacillin+Tazobactam (81.3%), [Table-8, Figure-2]. As, there were only 4 isolates of Acinetobacter spp., 3 each of Pseudomonas spp., and Proteus mirabilis and 2 of Citrobacter spp., their sensitivity /resistance pattern is tabulated as number of isolates of each species, sensitive or resistant [Table-9]. Among the gram positive isolates, Enterococcus spp. (12 isolates), recorded resistance to 75% of the isolates for Norfloxacin, followed by Penicillin (41.7%). All isolates were sensitive to Vancomycin and Linezolid (100%), with Chloramphenicol (91.7%) and Ampicillin (83.3%) coming close [Table-10, Figure-3]. Of the 6 Staphylococcus aureus isolates, there were no MRSA strains. Only Penicillin showed resistance to 50% of the strains. All the strains were sensitive to Clindamycin, Cloxacillin, Gentamicin, Linezolid, Rifampicin and Vancomycin (100%), with others, Norfloxacin, Cefazolin and Co-trimoxazole showing susceptibility to 83.3% of the isolates [Table-11, Figure-4]. There were also 7 multi-drug resistant isolates, of 4 from E. coli, 2 of Klebsiella spp. and 1was Acinetobacter sp. Four isolates of Candida spp., other than C. albicans and 1 Candida albicans were also isolated [Table-6].
Table 1: Sex wise distribution of UTI cases (n=168) 6
Table 2: Age wise distribution of UTI cases (n-168)
Table 3: Age wise distribution of UTI cases in male (n=40)
Table 4: Age wise distribution of UTI cases in female (n=128)
Table 5: Ward wise distribution of UTI cases (n=168) 7
KK- Peripheral multispeciality hospitals, OP- Out patient, MICU- Medical intensive care unit, PICU- Paediatric intensive care unit, PdW- Paediatric ward, ANW- Antenatal ward, FOW- Female obstetric ward, MMW- Male medical ward, FMW- Female medical ward, MSW- Male surgical ward, FSW- Female surgical ward, SICU- Surgical intensive care unit Table 6: Prevalence of pathogens among UTI cases (n=168)
Table 7: Antibiotic susceptibility pattern of Escherichia coli isolates (n=117)
Table 8: Antibiotic susceptibility pattern of Klebsiella spp. isolates (n=16)
S- sensitive; R- Resistant
Table 9: Antibiotic susceptibility pattern of Acinetbacter spp., Pseudomonas spp., Proteus mirabilis and Citrobacter spp
Table 10: Antibiotic susceptibility pattern of Enterococcus spp. isolates (n=12)
S- sensitive, R-resistant
Table 11: Antibiotic susceptibility pattern of Staphylococcus aureus isolates (n=6)
S-sensitive, R-resistant
Figure 1 Figure 2 Figure 3 Figure 4 Figure 1: Antibiotic susceptibility pattern of Escherichia coli isolates in % (n=117) Figure 2: Antibiotic susceptibility pattern of Klebsiella spp. isolates in % (n=16); Figure 3: Antibiotic susceptibility pattern of Enterococcus spp. isolates in % (n=12); Figure 4: Antibiotic susceptibility pattern of Staphylococcus aureus isolates in % (n=6)DISCUSSION Our study revealed an isolation rate of 16.8% (168 isolates) from the total 1000 suspected UTI cases (single organism from each of positive case). This observation is very close to another study from Jaipur, India, which reported 17.19% isolation rate 18. The predominance of female UTI cases (76.2%) over the male (23.8%), out of the total 168 confirmed UTI cases in this study, more or less correlates with another study from Odisha, India, which recorded 78.8% of female UTI cases and only 21.1% of male cases 19. The age group of >70 in male, accounted for the most number of UTI cases (32.5%) and among female, 21-30 age group recorded the maximum number of UTI cases (21%), followed by 31-40 age group (17.9%), in our study. This is in accordance with the study from Odisha, India 19, where they reported that 18-27 age group in female, possessed the highest number of UTI cases (29.2%), followed by 28-37 group (26.2%). Also, among male, >68 age group possessed the majority of the isolates (41.8%). This observation strengthens the previous documentations, that the fertility age group of 21-40 females are the most infected UTI cases, and the elderly immuno-depleted, >70 males are the mostly infected UTI group. Out of the confirmed UTI cases, 54.8% were from OPD and remaining 45.2% from IPD, in our study. This observation varies very much from another study from Nagaland, India, wherein, the authors reported a whopping 82.9% of UTI cases from OPD and a meager 17.1% from IPD 20. The predominance of Escherichia coli as the most isolated species among the UTI cases (69.6%), followed by Klebsiella spp. (9.5%), in our study, more or less correlates with a study in Patiala, Punjab 21, wherein the authors reported that E. coli was the most predominant isolate (67%), followed by Klebsiella spp. (14%). The isolation rate of Citrobacter spp. (1.2%), Proteus mirabilis (1.8%) and Enterococcus spp. (7.1%), in our study is more or less similar to that of a report from Bengaluru, India, wherein, the authors observed an isolation rate of, 1.3%, 1.8% and 9.4%, respectively 22. The isolation rate of Pseudomonas spp. (1.8%) and Staphylococcus aureus (3.5%), out of the total UTI cases in this study, varies a little bit from another study from Odisha, India, wherein, 1.6% and 4.9% respectively, was the isolation rate 19. Candida spp. isolation rate of 2.9% in our study differs from other studies elsewhere in India 20, 22. We have also reported 4 strains (2.4%) of Acinetobacter spp., as well, out of the 168 UTI cases. The increasing trend of resistance pattern of Escherichia coli isolates, for tested antibiotics, as, Amoxyclav (85.5% of isolates), Nalidixic acid (75.3%), Amoxicillin (73.5%), Cefuroxime (54.7%), Cefixime (53.8%), Cefotaxime (52.2%), Ciprofloxacin (46.2%) and Norfloxacin (40.2%), was reported in our study. By comparing this observation, Cefuroxime and Cefotaxime have slightly less percentage of resistance, as reported from a study in Jaipur, India, where it was, 66.67% and 70%, respectively 18. On the other hand, Amoxyclav and Nalidixic acid were showing higher levels of resistance of 80% and 94.6% respectively, in that study as do ours. Ciprofloxacin (74.8%) was again more resistant than our study. But, the antibiotics most sensitive reported in our study, being, Meropenem, Piperacillin+tazobactam, Amikacin and Gentamicin, more or less correlates with a study in Karnataka 23, there by ascertaining the earlier findings. In the case of Klebsiella spp. also, Amoxiclav (87.5%), turned out to be the most resistant drug in our study, which was very close to a finding from Patiala, Punjab, India (77.2%) 21, but, it was only 63%, registered in two other studies from Bhopal, India, and North West Pakistan 24,25. Only, 31,3% of the strains were resistant to Ciprofloxacin, whereas, it was 73.3% in the Punjab study 21. Cefuroxime and Cefixime reported 43.7% and 37.5% of the strains in our study, but, it was 76% for cephalosporins in general in that study 21. Co-trimoxazole recorded 37.5% resistance in our study, which was very less compared to another study in Gwalior, India, (76%), 26. Meropenem, Gentamicin, Amikacin and Piperacillin+Tazobactam remained the drugs of choice against Klebsiella spp. in our study. As for the 12 strains of Enterococcus spp. isolated, only Norfloxacin (75%) and Penicillin (41.7%) showed resistance, among the antibiotics tested, with Vancomycin, Linezolid and Chloramphenicol remained the drugs of choice. Among the 6 isolates of Staphylococcus aureus, only Penicillin showed resistance to 50% of the strains. Among the remaining species isolated, which were very few in number to make a resistance impact, only out of the 4 strains of Acinetobacter spp., isolated all 4 were resistant to Ampicillin, Amikacin, Amoxiclav, Amoxicillin, Cefotaxime and Cefixime. There was not much of resistance recorded among the other species. Apart from all these increased pattern of antibiotic resistance among E. coli and Klebsiella spp., especially, Amoxiclav, Ciprofloxacin and cephalosporins in particular, the matter of concern was the presence of 7 multi-drug resistant strains, 4 of E. coli, 2 of Klebsiella spp., and 1 of Acinetobacter sp. As a result, a periodic elucidation of antibiotic susceptibility pattern of all the urinary pathogens is a timely requirement, at least in this part of South Trivandrm district of Kerala, India, as there is no report of substance, like our study available, so far.
CONCLUSIONS Escherichia coli being the predominant isolate, showed the highest level of resistance to Ampicillin (93.2%), followed by Amoxiclav (85.5%), Nalidixic acid (75.3%), Amoxicillin (73.5%), Cefuroxime (54.7%), Cefixime (53.8%), Cefotaxime (52.2%), Ciprofloxacin (46.2%) and Norfloxacin (40.2%). Among Klebsiella spp., Ampicillin and Amoxiclav were the most resistant antibiotics (87.5%), followed by Amoxicillin (56.3%), Cefuroxime (43.7%) and Cefixime and Co-trimoxazole, 37.5% each. As for the 12 strains of Enterococcus spp. isolated, only Norfloxacin (75%) and Penicillin (41.7%) showed resistance, among the antibiotics tested. Among the 6 isolates of Staphylococcus aureus, only Penicillin showed resistance to 50% of the strains. Among the remaining species isolated, which were very few in number to make a resistance impact, only out of the 4 strains of Acinetobacter spp., isolated, all 4 were resistant to Ampicillin, Amikacin, Amoxiclav, Amoxicillin, Cefotaxime and Cefixime. Meropenem, Piperacillin+Tazobactam, Amikacin and Gentamicin remained the most sensitive drugs, in general, to act as reserve antibiotics to be instituted, in case of severe complicated cases of UTI. Apart from all these increased pattern of antibiotic resistance among E. coli and Klebsiella spp., especially for Amoxiclav, Ciprofloxacin and cephalosporins in particular, the matter of concern was the presence of 7 multi-drug resistant strains, 4 of E. coli, 2 of Klebsiella spp., and 1 of Acinetobacter sp. As a result, constant testing of uropathogens isolated then and there, for their ever changing antibiotic susceptibility pattern is the timely requirement, especially in the southern part of Trivandrum district, Kerala, India, like this study. Acknowledgements We are thankful to Dr. S Rema Devi, Professor and Head of the department of Microbiology, Dr. Somervell Memorial CSI Medical College and Hospital, Karakonam, Trivandrum dist., Kerala, India, for permitting me to carry out this work. Also, we are indebted to the Director and the Principal of our institution for their constant encouragement in research related activities.
REFERENCES
infection treated in a rural tertiary care hospital. Indian J Pharm Pract 2011;4:57‑63.
Policy for Articles with Open Access
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.