 Home
Home
|
Table of Content - Volume 17 Issue 3- March 2021
The utility of a single antistreptolysin O titer in the diagnosis of acute rheumatic fever at tertiary health care centre
Charushila S Halgarkar1, Madhumalti R Madavi2*, S L Nilekar3
1Assistant Professor, 2Junior resident, 3Professor, Department of Microbiology, Swami Ramanand Tirth Rural Medical College Ambajogai, Beed Maharashtra, INDIA. Email: madhumadavi31@gmail.com
Abstract Background: Rheumatic fever is delayed immune response to infection of group A haemolytic streptococci. RF affects millions of children in developing countries. Diagnosis of RF is done with Jone’s criteria which includes raised ASO titer. Present study focus on utility of single ASO titer. Aim and objective: To study the utility of a single Antistreptolysin O titer in the diagnosis of acute rheumatic fever at tertiary health care centre Methodology: Present study was a prospective study carried out in children diagnosed with rheumatic fever by Jone’s criteria. Data was collected was clinical history, clinical examination and Anti Streptolysin O titer in patients. Data was analysed with appropriate statistical tests. Results: Minimum age was 4 years and maximum was 15 years. Male to female ratio was 2.57:1. Majority of the patients 10 (40%) suffered from polyarthritis. Polyarthritis and carditis was observed in 20% patients. Lowest ASO titer found was 183 IU and highest ASO titer was 1522 IU. . Mean ASO titer in our study was 437.8± 62.64 IU. Lowest titers were observed in patients with chorea and Highest ASO titer was observed in patients with polyarthritis and carditis.
INTRODUCTION Rheumatic fever is an autoimmune disease developing after β-haemolytic Group A streptococcus infection. It is commonly observed in children and young adults.1 Rheumatic fever is prevalent in developing countries. It is estimated that there are about 15 million cases of rheumatic heart disease in the world. It contributed 2,33,000 deaths annually.2 India contributes to 25%–50% of the global burden of Rheumatic Heart Disease.3 Infections of beta haemolytic streptococci starts with pharyngitis. Later on it leads to damage to immune system of the host. Recurrent rheumatic fever leads to rheumatic heart disease sometimes progress to atrial fibrillation, embolic stroke and heart failure.4 Rheumatic fever is diagnosed with Jone’s criteria. It was developed by Dr T Duckett Jones and has been revised several times. It includes Major and minor criteria. Major criteria are carditis, polyarthritis, erythema marginatum, subcutaneous nodules and chorea. Minor criteria include fever, arthralgia and laboratory findings of elevated erythrocyte sedimentation rate, C-reactive protein and prolonged PR interval on ECG. Diagnosis of acute rheumatic fever is confirmed by presence of two major, or one major and two minor criteria with supporting evidence of antecedent group A streptococcal infection in the form of positive throat culture or elevated or rising anti-streptolysin titer.5 Beta haemolytic streptococci releases haemolytic exotoxins in host. Streptolysin O is one exotoxin released by them. Immune reaction in host leads to production of anti-steptolysin O (ASO) antibodies in the human serum.6 Streptococcal antibody tests are used for the diagnosis of infections caused by group A Streptococcus.7 The appearance of ASO in serum of patient or rise in ASO titer indicates recent streptococcal infection. When single specimen is available titer greater than upper limit of normal can be considered as prespumptive of streptococcal infection.8,9 Present study was conducted to study the utility of a single Antistreptolysin O titer in the diagnosis of acute rheumatic fever at tertiary health care centre. Aim and objective: To study the utility of a single Antistreptolysin O titer in the diagnosis of acute rheumatic fever at tertiary health care centre
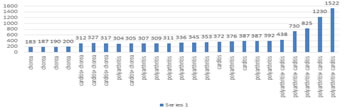
MATERIAL AND METHODS Present study was a prospective study carried out in department of Microbiology at a tertiary health care centre. Study population was children diagnosed with rheumatic fever, Inclusion criteria: 1. Children diagnosed with rheumatic fever using Duckett Jones criteria (Chorea, polyarthritis, carditis, subcutaneous nodules and erythema marginatum) Exclusion criteria: 1. Parents of children not willing to participate the children in study Study was approved by ethical committee of the institute. A valid written consent was taken from parents of the children after explaining study to them. Data was collected with pre tested questionnaire. Data included history of the patients and clinical examination. Through clinical examination was done. Duckett Jones criteria was used for diagnosis of acute rheumatic fever. Major criteria used were Chorea, polyarthritis, carditis, subcutaneous nodules and erythema marginatum. Children diagnosed as acute rheumatic fever were included in the study. Chorea, Polyarthritis and carditis were seen alone or in combination with each other in 25 patients. Subcutaneous nodules and erythema marginatum were not observed in any patients. All patients underwent Anti Streptolysin O titer. Serum concentration of ASO was estimated by semi-quantitative method based on lysis of RBCs14. Serum samples were inactivated by incubating at 56°C for 30 min in water bath. They were diluted (1:10) with phosphate-buffered saline (PBS) containing 0.1 per cent albumin. 0.5 ml of diluted sample was mixed with 4.5 ml of PBS with 0.1% albumin. Serial dilutions were prepared. In a tube 0.5 ml of reduced Streptolysin O (0.14 per cent sodium dithionite) was added. After gentle mixing, the tubes were incubated at 37°C for 15 min in water bath. A volume of 0.5 ml of erythrocyte suspension was added to each tube and mixed by gentle stirring. Finally, the tubes were incubated at 37°C for one hour. The ASO titre was calculated by haemolysis and the reciprocal values of their corresponding dilutions. Data was entered in excel sheet. Data was analysed with SPSS version 20. RESULTS After considering inclusion and exclusion criteria we studied 25 patients admitted in tertiary health care centre. In our study, majority of the patients were from the age group of 6- 10 years (40%) followed by 11-15 years (32%). Children in the age group 0-5 years were 28%. Minimum age was 4 years and maximum was 15 years. (table 1) In our study, out of 25 children 18 (72%) were male and 07(28%) were female. Male to female ratio was 2.57:1. (fig 1) Table 2 shows distribution of patients according to Jone’s major criteria. In our study, majority of the patients 10 (40%) suffered from polyarthritis. Polyarthritis and carditis was observed in 20% patients. Polyarthritis and chorea was observed in 4(16%) patients. chorea alone was observed in 4(16%) patients. Carditis alone was seen in 2(8%) patients. Fig 2 shows distribution of patients according to ASO tier and Jone’s major criteria. Lowest ASO titer found was 183 IU and highest ASO titer was 1522 IU. Mean ASO titer in our study was 437.8± 62.64 IU. Lowest titers were observed in patients with chorea. It ranged from 183 IU to 200 IU. Highest ASO titer was observed in patients with polyarthritis and carditis. Titer in patients with polyarthritis and carditis ranged from 483 IU to 1522 IU. All patients had titers above 300 IU except the patients with chorea alone
Table 1: Distribution of acute rheumatic fever patients according to age
Figure 1: Distribution of acute rheumatic fever patients according to sex
Table 2: Distribution of acute rheumatic fever patients according to Jone’s criteria
Figure 2: Distribution of patients according to ASO titer and jones major criteria
DISCUSSION In our study, majority of the patients were from the age group of 6- 10 years (40%) followed by 11-15 years (32%). Male to female ratio was 2.57:1. In our study, majority of the patients 10 (40%) suffered from polyarthritis followed by Polyarthritis and carditis (20%). Various factors play an important role in ASO levels. The upper limit of normal for ASO titer is affected by site of infection, season and geographical location. 10,11 Various studies has been carried out for ASO titers in acute rheumatic fever patients and normal children. Different studies in various geographic locations showed different ASO titers in normal children. In US ASO level was 240 IU/ml. The ASO levels were 200 IU/ml in Tanzania and 326 IU/ml in korea. In developing countries like India levels were 242/IU.8,12-14 Sethi S et al. studied Anti-Streptolysin O Titers in Normal Healthy Children of 5-15 Years and found the level 239 IU/ml.15 Karmakar et al. found upper level of ASO titer of 305 IU/ml.16 In our study, Mean ASO titer was 437.8± 62.64 IU. This ASO level is greater than upper normal limit in any geographic location. In our study, Lowest ASO titer found was 183 IU and highest ASO titer was 1522 IU. Lowest titers were observed in patients with chorea. It ranged from 183 IU to 200 IU. Highest ASO titer was observed in patients with polyarthritis and carditis. Titer in patients with polyarthritis and carditis ranged from 483 IU to 1522 IU. All patients had titers above 300 IU except the patients with chorea alone. Kotby et al. reported ASO titer of 215.4 IU/ml in RHD cases which was lower than that observed in healthy controls (245.09 IU).17 In a study by Ayoub EM et al., Anti streptolysin O titer in rheumatic children was significantly higher than non- rheumatic subjects.18 Romica AM et al. studied streptoccal infection and antistreptolins o titer in children and found that streptolysin O indicates recent streptococcal infection and not active rheumatic fever.19 In a study by Machado CS et al., they studied children with acute rheumatic fever, recurrent tonsillitis and Juvenile idiopathic arthritis. They followed all patients with ASO titers and concluded that ASO titers in Acute Rheumatic Fever indicates a significant response in the acute phase and helps to distinguish it from other diseases with high ASO titers.20 Borschmann ME et al. studied ASO titers in children with recurrent tonsillitis and concluded that ASO titers are helpful for differentiating the infectious agents. Group A beta haemolytic streptococcus infection showed raised titers.21 Kotby et al. studied different groups of children with stages of rheumatic fever and tonsillitis and found that children with acute rheumatic fever had significantly higher titers of ASO as compared to other groups. 17 ASO titer were higher in patients with acute carditis. By the time patient developes acute carditis the titers of ASO reaches it’s peak hence we observe higher levels in carditis patients. Rheumatic chorea developes in later stages and ASO level declines so we observe lesser levels in patients with chorea.17
CONCLUSION Single ASO titer is useful diagnostic tool in confirmation of acute rheumatic fever.
REFERENCES
Policy for Articles with Open Access
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.