 Home
Home
|
Table of Content Volume 16 Issue 1 - October 2020
Role of CT urography in evaluation of excretory tract pathologies
Shrikant Sharad Gundawar1*, Sudhir Navale2, Anand Rahalkar3, Sahil Kulkarni4
1Associate Professor, 2Professor, 4Jr III, Department of Radiology, Bharati Vidyapeeth Deemed University, Dhankawadi, Pune 411043, Maharashtra, INDIA.
Abstract Aim: To describe and establish the role of C.T. urography in evaluation of excretory tract pathologies. To assess the spectrum and prevalence of various excretory tract pathologies. Method and Material: The study included 100 patients referred to the dept. of Radiodaignosis of Bharati Vidyapeeth Medical College, Pune. Patients with suspected urinary tract pathologies, either based on clinical symptoms or ultrasound findings were include. Results: Among the 100 patients who underwent CT urography, 88 patients had pathological findings on CT urology, while 12 had no detectable abnormality. Conclusion: CT urography evaluates both renal paranchymal and urothetial pathologies in a single investigation. The entire spectrum of disorders affecting the urinary tract can be defected by CT urography and can be used as a one stop investigation in suspected urinary tract pathologies. Key Words: CT.
INTRODUCTION CT urography refers to the use of CT in complete evaluation of the urinary tract. CT is more accurate than conventional excretory urography (EU) in detection of renal and ureteric calculi, characterization of renal masses, assessing renal trauma and infections. CT has also become the imaging method of choice in evaluating patients with renal inflammatory diseases and hematuria1. The concept of CT urography is attractive since both the renal parenchyma and urothelium can be evaluated with a single comprehensive examination. Current investigations on multi-slice CT urography (MSCTU) focus on methods to improve opacification and distension of the upper urinary tract-the collecting systems, pelvis, ureters and bladder. Methods to reduce radiation exposure are being explored, including split-bolus contrast injection techniques that combine nephrographic and excretory phases into a single phase. It is likely that in the near future radiological evaluation of significant unexplained hematuria or of known or prior urothelial malignancy will consist of a single examination – MSCTU. CT urography initially referred to a combined (hybrid) examination using CT evaluation of the renal parenchyma, supplemented by a different method to evaluate the collecting systems and ureters, either digital CT radiograph or a full or partial set of EU radiographs. With the introduction of multislice CT (MSCT), the term CT urography now usually refers to the entire examination performed on a single CT examination (MSCTU). Single detector CTU was limited in its ability to detect small urothelial lesions and to complete the examination in a single breath-hold, but the improved resolution and speed of MSCT technology has resulted in remarkable axial and 3-D reconstructions that now challenge or even surpass the quality of EU images of the urothelium.
MATERIAL AND METHODS This was a prospective observational type of study done at Bharati Vidyapeeth and Deemed university, Pune. The study duration extended from September 2018 – August 2019. Total 100 patients were scanned with Philips 16 slice CT machine. All the patients referred for CT urography with hematuria and/or flank pain who were suspected clinically or by ultrasonographically to have urinary tract pathology. While the patients with renal failure who could not be given intravenous contrast, patients with contrast allergy were excluded from the study. After obtaining detailed history and the patients were asked to consume adequate amount of water prior to the study. After obtaining an initial supine AP scout film, contrast scan was done in supine position using 5mm collimation (100mA, 120Kv, pitch 6) from the domes of diaphragm to the base of the bladder. The patient was administered intravenously a bolus of 50 ml of 370mg/ml nonionic contrast. Immediately after the administration of IV contrast nephrographic phase was taken. Consequently after 15 min delayed images were obtained. Coronal and sagittal reformation of the images was done using maximal intensity projection (MIP), multiplanar reformation (MPR) and volume rendering technique (VRT) techniques. The axial as well as reformatted coronal and sagittal images were viewed on a workstation for evaluation.
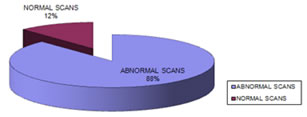
RESULTS Among the 100 patients who underwent CT urography, 88 had pathological findings on CT urography while 12 had no detectable abnormality. Chart No. 1
AGE DISTRIBUTION: Figure 1: No. of normal/Abnormal Patients Gender distribution of casesOf 100 cases studied, 65 cases (65.0%) were males and 35 cases (35.0%) were females. The male to female sex ratio in the entire study group was 1.9: 1.0.
Table 1
Age distribution of patients Table 2
The above observations denote that the present study has maximum number of patients in the age group of 31-45 years, followed by 45-60 years age group.
Table 3: Clinical symptomatology of patients in present study
The above table shows the clinical symptoms for which patients were referred for CT urography. Hematuria was the commonest indication for CT urography, followed by flank pain and dysuria. Patients who did not have any urinary tract symptoms but were referred after suspicious findings on USG have been included in the asymptomatic group. Spectrum of pathologies detected on CT urography Table No. 4
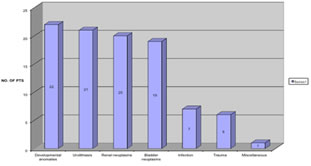
Chart 2: Spectrum of pathologies The above table and graph show that developmental anomalies were encountered most frequently and were closely followed by urolithiasis, bladder and renal neoplasms.
Table 5: Spectrum of developmental anomalies encountered
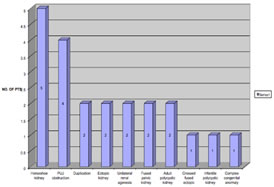
Chart 3: Developmental Anomalies This table and graph shows the frequency of developmental anomalies encountered. Horseshoe kidney and pelviureteric junction obstruction were most commonly seen anomalies.
Table 7: Distribution of renal neoplastic lesions
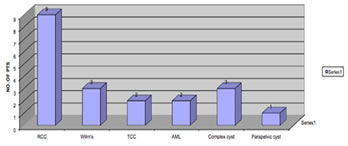
Chart 4: Distribution of neoplasma
The above chart shows that in the present study RCC was the commonest malignant tumor, followed by Wilm’s tumor. Among benign lesions, three complex cysts (two Bosniak class III and one class II cyst), and two angiomyolipomas were seen. Simple renal cysts were not included in this chart.
Table 8: Spread of malignant renal neoplasms
The above table shows venous invasion was seen in two cases each of all the three types of malignant renal tumors, while invasion of surrounding structures was present in three patients with Wilm’s tumor and in one patient with RCC. Distant metastases were present in one case of RCC and TCC each. Table 9:Staging of renal cell carcinoma (Robson’s criteria)
The above table shows that 44.4% patients with RCC undergoing CT urography were stage II, while 22.2% where stage IIIB. Table 10: Histopathological distribution of bladder malignancy
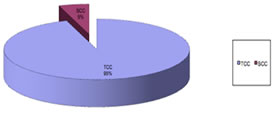
Chart 5: Histopathological distribution of bladder malignancies
This chart demonstrates that TCC was the commonest histopathological type of bladder malignancy encountered constituting 94.7% of the total, while only one case (that is 5.3%) was of squamous cell carcinoma.Table 8: Findings in patients with urinary tract trauma (n=6)
This chart demonstrates the distribution of findings in the 6 patients with urinary tract trauma who underwent CT urography parenchymal laceration and perinephric collection were most commonly encountered, both occurring in 83.3% of trauma cases. Parenchymal devascularization suggested by non enhancing areas were seen in 66.7% of the patients.
Table 9: Spectrum of findings in tuberculous infection of urinary tract (n=3)
This table demonstrates that pelvicalyceal thickening along with ureteric thickening and stricture were the most common findings and were noted in all three patients. Focal caliectasis was seen in two patients. The findings which were highly suggestive of tuberculous infection on CT urography were parenchymal and ureteric calcification. In case no.70 (as per the master chart), ureteric stricture and infundibular stenosis leading to phantom calyx was seen. Table 10: Distribution of calculus disease
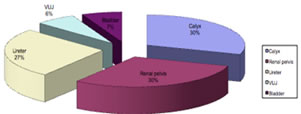
Chart 6: Distribution of Urolithiasis
This table and graph shows the distribution of calculus disease. Renal pelvic and calyceal calculi were the commonest, closely followed by ureteric calculi. Some patients had calculi at more than one site. USG had been done in all these cases but could not demonstrate ureteric calculi in five of these patients though variable degree of dilatation of the pelvicalyceal system was noted. USG also could not accurately detect the number of calyceal calculi in three patients. Ureteric calculi were radiolucent on plain radiograph in six of the patients while calyceal calculi were radiolucent in four patients.
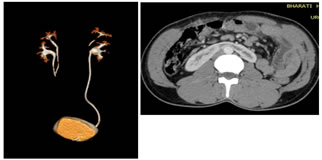
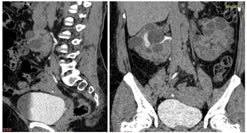
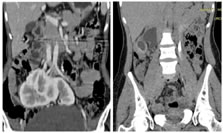
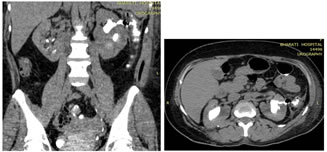
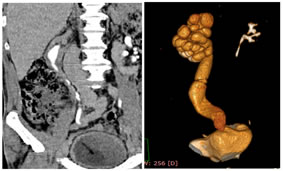
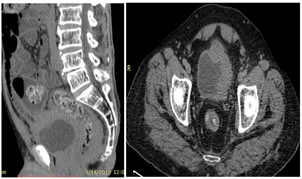
DISCUSSION During this prospective study, 100 patients with suspected pathology of the urinary tract, either based on clinical symptoms or ultrasound examination findings, underwent CT urography at Department of Radiodiagnosis, Bharati Vidyapeeth Medical College and Hospital, Pune, over a period of 12 months from September 2018 to August 2019. Out of the 100 patients referred for CT urography, 88 were found to have positive findings on CT urography. Male preponderance was seen. Maximum number of patients were in the age group of 31-45 years, followed by 45-60 years age group. Hematuria was the commonest indication for CT urography, followed by flank pain and dysuria. Spectrum of Pathologies in CT Urography The study conducted by Caoili et al. included 65 patients of which 5 had congenital anomalies, 5 urolithiasis, 34 renal lesions and bladder abnormalities were present in 25. Lin et al. studied 102 patients among whom the distribution of pathologies included 4 congenital anomalies, 40 urolithiasis, 24 renal masses and 29 inflammatory lesions. Among the 100 patients in our study developmental anomalies (22), urolithiasis (21), renal tumors (20) and bladder abnormalities (19) were almost equally distributed. In addition, 6 patients of trauma and 7 of urinary tract infection were also included. One patient had a reno-colo-cutaneous-fistula. Congenital anomalies CT urography beautifully depicts most anomalies of renal position, number, and form. The exact orientation and position of the ureters and pelvicalyceal system can be determined. The superior z-axis reconstructions with multidetector CT aid in obtaining high diagnostic quality three dimensional reconstructions, particularly in the coronal plain (Kalra et al. ). In our study two cases of pelvicalyceal and ureteric duplication were present, one bilateral (Fig 1 ) and the other unilateral. With complete opacification the exact extent of duplication and ectopic ureteric opening if present, could be visualized. Of the five cases of horseshoe kidney (Fig 2), two had obstructing pelvic calculi which had caused dilatation of the pelvicalyceal system In these two patients the exact localization of calculus in the distorted pelvicalyceal system could be achieved by CT urography. The other developmental abnormalities encountered included renal agenesis, adult polycystic kidneys (Fig 3), polycytic kidneys with retrocaval ureter on right side (fig. 4,5) fused pelvic kidneys (Fig 6) and pelviureteric junction obstruction. (Fig 7) Image 1 Image 2
Image 3 Image 4 Image 5 Image 6 Image 7 RENAL CALCULI In our study, we were able to identify accurately urolithiasis in all 21 patients. In five patients, ureteric calculi which could not be detected on USG were diagnosed using CT urography. All these patients however had some degree of dilatation of the proximal collecting system on ultrasound. CT urography also could detect more number of calyceal calculi than was evident on USG in three patients. CT urography was easily able to detect calculi which were radiolucent on abdominal radiograph. RENAL TRAUMA CT urography provides critical anatomic and physiological information that determines management of trauma to the urinary tract. It helps in accurate evaluation of the type and severity of parenchymal injury, pelvicalyceal disruption, the extent of perirenal hemorrhage and parenchymal devascularization, and the presence of major injuries to the vascular pedicle. In addition, it aids in confirming the presence of urinary extravasation and depicts occult kidney diseases (Kalra et al.3). One patient had iatrogenic renal parenchymal injury during percutaneous nephrostomy. This patient had an obstructing pelvi- ureteric calculus and while pigtail insertion the parenchymal injury resulting in a reno-colo-cutaneous fistula. (Fig 8,9). Image 8 Image 9 INFECTION: In our study in one patient had pyogenic infection had resulted in formation of a renal abscess.(fig 19) In chronic gram negative infection of the urinary tract CT urography beautifully demonstrated ureteric thickening due to the infection. The distensibility of this thickened segment was maintained(fig 10). Where in case of stricture distensibility is lost and pre stricturous dilatation is seen. (Fig 11). Spectrum of findings in TB infections of urinary tract showed, Pelvicalyceal thickening along with ureteric thickening and stricture as the most common findings followed by focal caliectasis. Parenchymal and ureteric calcification, was also seen. Image 8 Image 9 CT urography is superior to both IVU and ultrasonography in the assessment of kidney infection (Rauschkolb et al. , Hoddik et al. , Soulen et al. ). Although routine renal imaging is not indicated in uncomplicated renal infections, CT urography is often helpful in patients when complications like abscess formation intervene. Gas, calculi, renal parenchymal calcifications and hemorrhage are well demonstrated on plain CT. A striated nephrogram maybe seen in acute pyelonephritis. Hypodense areas with obliterated corticomedullary differentiation maybe present. Other features of infection include enlargement of the kidney, thickening of the pelvicalyceal walls and fascial thickening (Kawashima et al. ). Parenchymal abnormalities are best seen in the nephrographic phase. NEOPLASTIC
Image 8 Image 9
SUMMARY Multidetector CT urography with its superior spatial resolution, higher speed and isotropic reconstruction capability is an effective investigation for urinary tract disorders. Developmental anomalies of the urinary tract along with their complications are very well depicted by CT urography. CT urography is very useful in the early detection, evaluation and staging of renal parenchymal and urothelial malignancies. CT urography precisely grades urinary tract trauma playing a crucial role in the management of such patients. In urolithiasis, CT urography has very high sensitivity, with plain CT accurately detecting calculus disease in all the patients. CT urography plays an important role in detecting the features as well as complications of both tuberculous and pyogenic infections of the urinary tract
CONCLUSIONSCT urography evaluates both the renal parenchymal and urothelial pathologies in a single investigation. The entire spectrum of disorders affecting the urinary tract can be detected by CT urography. CT urography has the potential to become a one stop investigation for urinary tract pathologies.
REFERENCES
Policy for Articles with Open Access: Authors who publish with MedPulse International Journal of Radiology (Print ISSN: 2579-0927) (Online ISSN: 2636-4689) agree to the following terms: Authors retain copyright and grant the journal right of first publication with the work simultaneously licensed under a Creative Commons Attribution License that allows others to share the work with an acknowledgement of the work's authorship and initial publication in this journal. Authors are permitted and encouraged to post links to their work online (e.g., in institutional repositories or on their website) prior to and during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work.
Height, IVDL-Intervertebral Disc Length
Policy for Articles with Open Access
Authors who publish with MedPulse International Journal of Radiology(Print ISSN: 2579-0927) (Online ISSN: 2636 - 4689) agree to the following terms: Authors retain copyright and grant the journal right of first publication with the work simultaneously licensed under a Creative Commons Attribution License that allows others to share the work with an acknowledgement of the work's authorship and initial publication in this journal. Authors are permitted and encouraged to post links to their work online (e.g., in institutional repositories or on their website) prior to and during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work. |
|

 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.