 Home
Home
|
Table of Content Volume 16 Issue 1 - October 2020
A study of ultrasonographic findings in ovarian tumours
Purushothama Raju N
Associate Professor, Department of Radiodiagnosis, The Oxford Medical College And Research Centre, Yadavanahalli, Bengaluru, INDIA. Email: drraju_17@hotmail.com
Abstract Background: Ovarian cancer is the second most common gynecologic malignancy and is the fifth leading cause of cancer death in women. ovarian cancer present with advanced stage disease, which is associated with a poor prognosis. Ultrasonography is easy, non invasive tool used for diagnosis of ovarian masses. Aim and objective: To study the ultrasonographic findings in ovarian tumours Methodology: Present study was a cross sectional study carried out in all patients with clinically suspected ovarian masses from department of OBGY and referred to department of radiology for ultrasonography. Data was collected with pretested questionnaire. Data included demographic data, clinical history and clinical examination. All patients were subjected to transabdominal ultrasonography with full bladder technique with 2 to 5 MHz probe. Data was analysed with appropriate statistical tests. Results: In our study, Maximum number of cases (31%) were seen in 30-39 years age group followed by 25% in 40-49 years age group. Most commonly observed clinical feature was lump in abdomen (65%) followed by pelvic pain (13%). Size of the tumour, thick wall, multilocularity, septal thickness and calcification were significantly associated with malignancy (p<0.001). Key Word: ovarian tumours.
INTRODUCTION Ovarian cancer is one of the leading cancers in Indian women. In most of the population-based cancer registries in India, ovarian cancer is the third leading site of cancer among women after cervix and breast cancer. The age-adjusted incidence rates of ovarian cancer vary between 5.4 and 8.0 per 100,000 population in different parts of the country.1 Ovarian tumours can be classified based on cells of their origin into epithelial, sex cord stromal, germ cell and metastatic types. Most commonly observed tumour is epithelial tumors counting about 85% to 90% of all ovarian malignancies. Histologic subtypes in epithelial ovarian cancer include serous, mucinous, endometrioid, clear cell, and undifferentiated tumors. The major risk factor is the family history. Other associated risk factors are excess body weight, Height, Cigarette smoking and Physical inactivity. 2,3 More height may be related to genetic and environmental factors including growth hormone exposure during early life. Physical inactivity is associated with about a 30% higher risk of epithelial ovarian cancer.4-6 The International Agency for Research on Cancer has observed that perineal use of talc-based body powder increases the risk of ovarian cancer but evidence is limited. 7Ovarian tumours have poor prognosis. The overall 5-year survival is approximately 45%, primarily due to the late stage at diagnosis of the disease. 8 Ultrasonography is a relatively simple and noninvasive diagnostic method that provides clinicians with useful information relevant for determining the optimal management strategy for a given patient. Previous studies found that ultrasonography has 88%-96% sensitivity and 90-96% specificity for detecting ovarian tumours.9-11 Benign ovarian tumours are best treated conservatively but suspected malignant masses should be referred to specialized units for further management. Ultrasound is important for early detection of ovarian tumours and it can be a guide for further management. Present study was conducted to study the ultrasonographic features of ovarian tumours.
MATERIAL AND METHODS Present study was a cross sectional study carried out at department of radiology at a tertiary health care centre. Study population was all patients with clinically suspected ovarian masses from department of OBGY and referred to department of radiology for ultrasonography. A total of 100 patients diagnosed clinically with ovarian mass were studied. Inclusion Criteria: 1.All patients with solid ovarian mass detected clinically and ultrasound examination 2.All patients with cystic ovarian lesions more than 6 cms. Exclusion criteria: 1.Ovarian cyst less than 6 cms with clear cysts in reproductive age group.2. Patients not willing to participate in the study Study was approved by ethical committee of the institute. A valid written consent was taken from the patients after explaining study to them. Data was collected with pretested questionnaire. Data included demographic data and clinical history. Detailed Clinical history, menstrual history, obstetric history were noted. A through clinical examination was done. All patients underwent routine investigations like complete blood count, renal function tests, liver function tests, random blood sugar etc. All above data was recorded from OBGY department. All patients were subjected to transabdominal ultrasonography with fu’ll bladder technique with 2 to 5 MHz probe. If required Transvaginal Sonography with empty bladder technique with 6.5MHz was done. Ultrasonography was done with ALOKA prosound Alpha 7 Diagnostic Ultrasound System. Ultrasound examination included size, shape, echogenicity of the ovarian lesion in sagittal and transverse planes, Wall thickness, locularity of the lesion and calcification. Histopathological follow up of all cases taken for correlating the ultrasonography. Data was subjected to statistical analysis using Statistical package for social sciences (SPSS v 21.0, IBM).
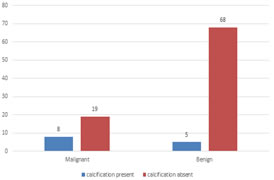
RESULTS In our study, Maximum number of cases (31%) were seen in 30-39 years age group followed by 25% in 40-49 years age group. Out of 100 patients, 81% had unilateral involvement of ovary. Only 29% had bilateral involvement. Out of 100 patients, only 4% had positive family history. Remaining 96% had no significant family history. Out of 100 patients, 61% patients were in premenopausal age group and 49% were in postmenopausal age group. Table 1 shows distribution of patients according to clinical features. Most commonly observed clinical feature was lump in abdomen (65%) followed by pelvic pain (13%). Pain in abdomen and distension of abdomen was observed in 12% and 10% patients respectively. Table 2 shows distribution of study subjects according to benign and malignant ovarian masses diagnosed by USG and histopathology. On ultrasonography 64% masses were benign and 36% masses were malignant. On histopathology, 73% masses were diagnosed as benign and 27% were malignant. (table 2) Among the malignant tumour, 74.07% tumours were of size ≥10 cm and 25.92% tumours were of the size < 10 cm. in case of benign tumours, out of total 73 tumours 95.89% tumours were of size less than 10 cm and 4.1% tumours were ≥10 cm in size. Thus size of the tumour was significantly associated with malignancy (p<0.001 ). (table 3) Out of 100 lesions, 73 (71%) were cystic in nature. Out of these 73 lesions, 65(91.55%) were benign on histopathology. Remaining 6(8.45%) were malignant in nature. Out of 100 lesions, 23 (23%) were mixed in nature. Out of these 23 lesions, 17 (73.91%) were malignant on histopathology. Remaining 6 (26.09%) were benign in nature. Out of 100 lesions, only 6(6%) were solid in nature. Out of these 6 lesions, 4(66.67%) were malignant on histopathology. Remaining 2 (33.33%) were benign in nature. (table 4) Out of 100 lesions, 6 were solid in nature so 94 were included in table 5 for thickness. Out of 96 lesions 23 were with thick wall and 71 were thin walls. Among the 23 thick wall lesions, 21(91.3%) were malignant and 2(8.7%) were benign. Among the 71 thin wall lesions 02(2.82%) lesions were malignant and 69(97.18%) were benign. P value was < 0.001, highly significant suggesting that there exists a strong correlation between wall thickness of a lesion and risk of malignancy. (table 5) Out of total 100 lesions, 6 lesions were solid in nature on USG we included 94 lesions in locularity calculation table. Out of the rest 94 lesions, 78 lesions were multilocular. 57 (73.07%) of these lesions came out to be benign on histopathology. Rest 21(26.93%) were malignant. 16 lesions out of 94 lesions were unilocular. 14 (87.5%) of these lesions came out to be benign on histopathology. Only 2(12.5%) was malignant. P value was 0.01 (< 0.05) i.e. significant, which meant that multilocularity and malignancy have a positive correlation.(table 6) Out of the total 100 lesions, 12 were solid and 16 were unilocular , so we included 78 lesions for septal thickness. Out of these 78 lesions, 53 lesions showed thin septations (max thickness < 3mm) and 25 lesions showed thick septations (max thickness ≥ 3mm). 19 (76%) of 25 lesions showing thick septae turned out to be malignant on histopathology. Remaining 6(24%) lesions were benign. 51 (96.23%) out of 53 lesions which showed thin septae were found to be benign on histopathology. However, 2 (3.77%) were malignant on histopathology. From the table 7, it is clear that there is a strong correlation between septal thickness and malignancy- thicker the septae, more likelier chance of malignancy it is (p value <<0.05). Out of the total 100 lesions, calcifications were seen within 13 (13%) lesions only. Out of these 13 lesions, 8(61.53%) lesions were found to be malignant on histopathology. Rest 5 (38.47%) lesions came to be benign. Remaining 87 lesions did not show evidence of calcifications. 68(78.16%) and 19(21.84%) of them came out to benign and malignant respectively. P value < 0.05 significant meaning there exists a strong correlation between presence of calcification and malignancy. (fig 1)
Table 1: Distribution of ovarian tumour patients according to clinical features
Table 2: Distribution of study subjects according benign and malignant ovarian masses diagnosed by USG and histopathology
Table 3: Distribution of ovarian tumour patients according to size of tumour
Table 4: Distribution of ovarian tumour patients according to morphology
Table 5: Distribution of ovarian tumour patients according to wall thickness
Table 6: Distribution of ovarian tumour patients according to locularity
Table 7: Distribution of ovarian tumour patients according to septal thickness
Figure 1: Distribution of ovarian tumour patients according to calcification
DISCUSSION In our study, Maximum number of cases (31%) were seen in 30-39 years age group followed by 25% in 40-49 years age group. Similarily Khurana and Satia found 50 mean age of the patients was 37 years. 12 Most commonly observed clinical feature was lump in abdomen (65%) followed by pelvic pain (13%). Sehgal N (2019) in her study of 60 patients diagnosed with ovarian masses found that abdominal swelling (63%) and pain (60%) were the most common presenting symptoms.13 In our study, Out of 100 patients, 61% patients were in premenopausal age group and 49 % were in postmenopausal age group. Mohammad Momen Gharibvand (2018) in his study of 67 patients noted that premenopausal women had 36(53%) benign and 7 (10%) malignant pathology and postmenopausal women had 22(32.8%) benign and 2(2.9%) malignant pathology (P = 0.360). 14 In our study the correlation between size ≥10 cm and malignancy was statistically highly significant(p value <<0.05).In a study conducted by Minaretzis D et al.. in which they studied 959 patients with ovarian tumors retrospectively showed that significant increase in risk of malignancy was observed in tumors with maximum diameter of > 9 cm. 15 We found most common feature was mixed (i.e. cystic with a solid component) in malignant tumours. The most common feature in benign neoplasms was cystic. In accordance with our study, Khurana and Satia in their study of 50 patients with ovarian masses found that 71.4% of the benign tumors were cystic and 78% of the malignant tumors were mixed on grayscale morphology. 12 A strong correlation exits between wall thickness of a lesion and risk of malignancy. Similarly, Sassone et al.. (2001) in their study they found that thick wall was associated with 13 cases of ovarian malignancies out of 14 with difference being statistically significant. 16 A strong correlation exists between septal thickness and malignancy- thicker the septae, more likelier chance of malignancy it is (p value <<0.05). Ekerhovd E et al.. found that echo free unilocular cysts were having low malignancy risk. 17 In our study, presence of thick septation was more likely to be associated with malignant ovarian lesions and thin was in benign lesions and there was statistically significant difference in benign and malignant lesions for presence of thin and thick respectively with p value < 0.05. Similar findings were seen in a study by Douglas L Brown et al.. .18 In our study we found a strong correlation between presence of calcification and malignancy. Similarly, G J C Burkill et al.. concluded that ovarian tumors have a 8% prevalence of calcifications and were noted in total of 8% patients and more common in serous cystadenocarcinoma. 19 Conclusion
REFERENCES
Policy for Articles with Open Access: Authors who publish with MedPulse International Journal of Radiology (Print ISSN: 2579-0927) (Online ISSN: 2636-4689) agree to the following terms: Authors retain copyright and grant the journal right of first publication with the work simultaneously licensed under a Creative Commons Attribution License that allows others to share the work with an acknowledgement of the work's authorship and initial publication in this journal. Authors are permitted and encouraged to post links to their work online (e.g., in institutional repositories or on their website) prior to and during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work.
Height, IVDL-Intervertebral Disc Length
Policy for Articles with Open Access
Authors who publish with MedPulse International Journal of Radiology(Print ISSN: 2579-0927) (Online ISSN: 2636 - 4689) agree to the following terms: Authors retain copyright and grant the journal right of first publication with the work simultaneously licensed under a Creative Commons Attribution License that allows others to share the work with an acknowledgement of the work's authorship and initial publication in this journal. Authors are permitted and encouraged to post links to their work online (e.g., in institutional repositories or on their website) prior to and during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work. |
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.