 Home
Home
|
Table of Content Volume 16 Issue 1 - October 2020
Bronchial artery embolization at a tertiary care center- our experience with 52 patients
Yadav Waghaji Munde1, Prathamesh Bongale2, Sudhir Navale3*, Pragya Dixit4
1Associate professor, 3Professor, Department of Interventional Radiology, Bharati Vidyapeeth medical college, Pune-411043, INDIA. 2Managing Director, Indocare Diagnostics, Pune, INDIA. 4Associate consultant, Department- Interventional Radiology, Ruby Hall Clinic, Pune, Maharashtra, INDIA. Email: yadavmunde@gmail.com
Abstract Background: Hemoptysis is defined as the expectoration of blood from the lung alveoli or airways of the lower respiratory tract. The currently available approaches for patients with hemoptysis are conservative medical treatment, bronchial artery embolisation (BAE) and surgery. Advances in medical imaging, fiberoptic technology, and interventional radiology have improved patient outcomes and reduced mortality, bronchial artery embolization (BAE) has emerged as an effective minimally invasive means to control massive hemoptysis. In present study we studied bronchial artery embolization at our tertiary care hospital with regards to indication, procedure outcome and complications. Material and Methods: : Present study was a prospective, observational study conducted in patients with recurrent hemoptysis, not controlled by medical therapy, referred for bronchial artery embolization underwent BAE for hemoptysis. Results In present study 52 patients underwent BAE at our hospital. 27 % patients had severe life threatening hemoptysis at presentation while remaining 73 % patients had mild to moderate recurrent hemoptysis. Tuberculosis and it’s sequelae (46%) was most common cause. Other major causes were bronchiectasis (15%), acute infections (12%) and tumors / malignancy (10%). On radiological imaging we noted that bilateral involvement (48%) was more common followed by right side (31%) and left side (21 %) involvement. After identification of abnormal blush or bleeding vessel we embolised it. The number of arteries embolized per session were zero to four (mean ± SD=1.39 ±1.13 ). Right intercostobronchial (56%) was the most common culprit artery in our study followed by left bronchial (19%), common bronchial (17%) and right bronchial (13%). In present study initial success rate of BAE was 83% and the recurrence rate for bleeding at the end of 12 months was 17%. 1 patient had bronchial artery dissection, was minor dissection, no additional measures were needed. Conclusion: BAE is a safe and effective procedure that can be performed routinely in patients presenting with hemoptysis. It has an excellent short-term success rate and an acceptable long-term success rate. The success of BAE procedure depends on operator's skill, bronchial anatomy and hemoptysis etiology. BAE can be considered an acceptable alternative therapy for surgery in high risk patients. Key Words: Hemoptysis, tuberculosis, bronchial artery embolization
INTRODUCTION Hemoptysis is defined as the expectoration of blood from the lung alveoli or airways of the lower respiratory tract. Severity of hemoptysis is usually classified based on the amount of blood expectorated in 24 h. Hemoptysis is classified as mild (<30 ml), moderate (31–100 ml), severe (100–600 ml), and massive.1 Nowadays concept of massive hemoptysis is challenged by more significant clinical factors such as the briskness of bleeding, ability of a patient to maintain a patent airway and expectorate blood, the swiftness of available therapeutic options, and the patient’s underlying physiological reserve. The most common causes of hemoptysis vary based on the geographic location of the patient. In India, the most common causes of hemoptysis are tuberculosis, acute respiratory tract infections, chronic obstructive pulmonary disease, malignancy, and bronchiectasis. Hemoptysis without a known cause despite extensive investigation by both CT and bronchoscopy is termed “cryptogenic hemoptysis” and accounts for approximately 20% of patients initially presenting with hemoptysis.2 The currently available approaches for patients with hemoptysis are conservative medical treatment, bronchial artery embolisation (BAE) and surgery.3 The treatment of choice depends largely on the severity and urgency of the circumstances. Advances in medical imaging, fiberoptic technology, and interventional radiology have improved patient outcomes and reduced mortality, bronchial artery embolization (BAE) has emerged as an effective minimally invasive means to control massive hemoptysis.4 In present study we studied bronchial artery embolization at our tertiary care hospital with regards to indication, procedure outcome and complications.
MATERIAL AND METHODS Present study was a prospective, observational study conducted in patients underwent BAE for hemoptysis. Study was conducted in department of interventional radiology, Bharati vidyapeeth medical college and hospital. Study period was 2 years (from June 2018 to May 2020). Study protocol was approved by institutional ethics committee. Inclusion criteria Patients with recurrent hemoptysis, not controlled by medical therapy, referred for bronchial artery embolization. Exclusion criteria Deranged renal function; Coagulopathy; Cases with spinal artery originating from the culprit bronchial artery,
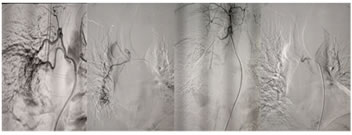
Clinical records were analyzed for symptoms, duration of hemoptysis and the basic disease. Chest radiographs and computed tomography (CT) images were analyzed for evaluation of etiology and lateralization of abnormalities. In non-emergency situation, before the embolization, culprit vessel is routinely identified in the CT angiography. The procedure is usually performed via a femoral route. After obtaining arterial access, flush aortogram was obtained to search for bronchial or intercostal arteries supplying the diseased lung parenchyma. With the help of a descending thoracic aortogram, the exact anatomical location of bronchial arteries was detected. Next, selective bronchial artery angiography was performed. Abnormal angiographic findings such as vessel enlargement and tortuosity, parenchymal blushing, shunting to PA or vein, aneurysm and contrast extravasation confirm the culprit vessel. Cannulation of the culprit vessel was performed with the help of a 0.014- 300 cm length wire followed by the advancement of microcatheter. Catheter-4 French cobra was used in most of the cases, few cases SIM1 catheter was used. Embolic material used was Polyvinyl alcohol (PVA) particles 500 micron. During BAE, in the absence of an identified bleeding site, several sensitive findings can localise the bleeding source; these include vascular hypertrophy and tortuosity, neovascularity, hypervascularity, aneurysm formation and shunting (bronchial artery to pulmonary vein or bronchial artery to pulmonary artery). Follow up was kept for 12 months. The normally distributed continuous data, expressed as the mean ± the standard deviation (SD) and percentages. Statistical analysis was done using descriptive statistics. During BAE, in the absence of an identified bleeding site, several sensitive findings can localise the bleeding source; these include vascular hypertrophy and tortuosity, neovascularity, hypervascularity, aneurysm formation and shunting (bronchial artery to pulmonary vein or bronchial artery to pulmonary artery). Follow up was kept for 12 months. The normally distributed continuous data, expressed as the mean ± the standard deviation (SD) and percentages. Statistical analysis was done using descriptive statistics. Figure 1: CASE1: Bronchial artery embolisation in a case of pulmonary koch's. A-Bronchial angiogram showed hypertrophied two bronchial arteries with common trunk on right side with abnormal blush in right lower lobe.
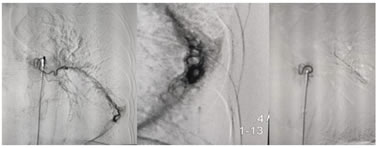
Figure 2: CASE 2: Left bronchial artery embolisation in a case of bronchiectasis. A-Hypertrophied bronchial artery with significant blush in left lower lobe. B-The magnified view of blush in left lower lobe. C-Post embolisation with PVA particles with patent stump.
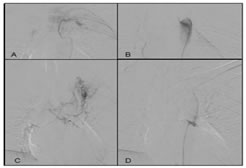
Figure 3: CASE3: Left upper lobe mass in 23 years female, causing recurrent hemoptysis. Angiogram showed mass supplied by a left 2nd intercostal artery and Hypertrophied bilateral bronchial arteries with common origin. The culprit vesels were embolised selectively by 500 micron PVA particles. Patients hemoptysis stopped completely.
RESULTS In present study 52 patients underwent BAE at our hospital. 27 % patients had severe life threatening hemoptysis at presentation while remaining 73 % patients had mild to moderate recurrent hemoptysis. Tuberculosis and it’s sequelae (46%) was most common cause. Other major causes were bronchiectasis (15%), acute infections (12%) and tumors / malignancy (10%). On radiological imaging we noted that bilateral involvement (48%) was more common followed by right side (31%) and left side (21 %) involvement. Table 1: Etiology of hemoptysis
After identification of bleeding vessel we embolised it. The number of arteries embolized per session were zero to four (mean ± SD=1.39 ±1.13 ). Right intercostobronchial (56%) was the most common culprit artery in our study followed by left bronchial (19%), common bronchial (17%) and right bronchial (13%).
Table 2: Major arteries involved.
In present study initial success rate of BAE was 83% and the recurrence rate for bleeding at the end of 12 months was 17%. 1 patient had bronchial artery dissection, was minor dissection, no additional measures were needed.
Table 3: Complications during bronchial artery angiography.
Ozgül MA, Turna A, Yildiz P, Ertan E, Kahraman S, Yilmaz
DISCUSSION In fatal hemoptysis, the inciting cause of death is not hemorrhagic shock, but asphyxiation from inability to oxygenate or ventilate because of hemorrhage flooding the airways. The total volume of the conducting airways averages 150 mL in adults.5 Therefore, a given hemorrhage that may be regarded as mild from another location can briskly become life threatening in the airways. Pulmonary tuberculosis continues to be a major public health burden in developing countries. Tuberculosis still remains the most common cause of hemoptysis as evident from recently reported studies from India.6,7,8 Similar finding was noted in present study. Structural damage caused by tubercular bacillus can subsequently result in pooling of secretions and infections, resulting in hemoptysis in patients with inactive tuberculosis.8 Despite adequate treatment, the disease while healing produces fibrosis, cavitation, and calcification leaving permanent sequelae in the lungs. Hemoptysis can be a result of a variety of sequelae and complications such as fibrosis or cicatrization, cavities, end-stage lung destruction, aspergilloma; airway lesions (including bronchiectasis, tracheobronchial stenosis, and broncholithiasis), or vascular lesions (including pulmonary or bronchial arteritis and thrombosis, bronchial artery dilatation, and Rasmussen aneurysm).9 BAE involves the identification of bronchial and systemic arteries feeding the diseased lung parenchyma using diagnostic angiography. Once identified, these are embolized using polyvinyl alcohol (PVA) particles, gel foam pledgets, or glue after selective catheterization. The value of BAE in controlling massive hemoptysis is well documented.10,11 Initially, use of BAE was advocated primarily for management of massive hemoptysis. However, increasingly it is used in moderate hemoptysis and recurrent mild hemoptysis that hampers the lifestyle of the patient. 10,11A variety of embolization agents can be used such as 300 to 600 mm polyvinyl alcohol particles, trisacryl gelatin microspheres, N-butyl cyanoacrylate glue, gelatin sponges, and metallic coils to occlude the bronchial vascular supply. Although there are many causes of hemoptysis, life-threatening hemoptysis requiring intervention most often occurs in the setting of chronic inflammatory lung disease, predominantly in cases of pulmonary tuberculosis (TB) and bronchiectasis.12 The surgical and endovascular therapeutic modalities are main treatment options with success rate of 85 to 100 percent in endovascular method and relatively lower in surgical modality with recurrence rate of 10 to 33 percent.13 In a systematic review of BAE, Panda et al.14 examined 22 studies totaling 3,265 patients and defined the initial success rate of BAE from 70% to 99%. However, the recurrence rate for bleeding is high, estimated up to 58% within 30 days. In present study initial success rate of BAE was 83% and the recurrence rate for bleeding was 17%. Inconsistent rebleeding rates have been reported in different studies. Fruchter et al.. reported bleeding recurrence in 57.7% of patients after successful BAE.15 Risk factors for recurrence post-BAE include bleeding from aspergillomas, TB, bronchiectasis, nonbronchial systemic collateral circulation, and bronchopulmonary shunting.14,15 BAE failure can be caused by recanalization of embolized arteries, incomplete embolization of existing arteries, and development of new collateral blood supply.15 In these cases, BAE should be considered as a temporary and adjuvant therapy to surgery or as a specific medical therapy. Shigemura et al..,16 reported immediate success in controlling hemoptysis in 88% of cases in a series of 55 patients. Of those, 70% had no evidence of recurrence after one year of follow-up. Joseph T et al..,17 noted 82.05% first-line success rate of BAE, while the long-term success rate was 89.47%, without statistical difference. Long term recurrence of haemoptysis was seen in 10.52% of cases. Ittrich et al..18 in their narrative review of BAE, have emphasized the operator's experience and how the “profound knowledge of bronchial anatomy” was related to procedural success. Complications of BAE include spinal cord injury, subintimal dissection of the aorta leading to mediastinal hematoma, arterial perforation by a guide wire, transient thoracic pain, shoulder pain and dysphagia.19 Minor complications were noted in present study. Multidetector row computed tomography (MDCT) is useful for visualizing bronchial arteries and detecting ectopic origins, particularly when the patient is aged and has a tortuous aorta and/or extensive arteriosclerosis.20 BAE has emerged in recent years as a treatment for severe, life-threatening hemoptysis, and has revolutionized the management of the disease, providing a reliable, minimally invasive tool with excellent diagnostic and therapeutic outcomes. 21 Present study was a single institute based study with small sample size. Further studies with larger sample size are required to attain more definite results.
CONCLUSION BAE is a safe and effective procedure that can be performed routinely in patients presenting with hemoptysis. It has an excellent short-term success rate and an acceptable long-term success rate. The success of BAE procedure depends on operator's skill, bronchial anatomy and hemoptysis etiology. BAE can be considered an acceptable alternative therapy for surgery in high risk patients.
REFERENCES
Policy for Articles with Open Access: Authors who publish with MedPulse International Journal of Radiology (Print ISSN: 2579-0927) (Online ISSN: 2636-4689) agree to the following terms: Authors retain copyright and grant the journal right of first publication with the work simultaneously licensed under a Creative Commons Attribution License that allows others to share the work with an acknowledgement of the work's authorship and initial publication in this journal. Authors are permitted and encouraged to post links to their work online (e.g., in institutional repositories or on their website) prior to and during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work.
Height, IVDL-Intervertebral Disc Length
Policy for Articles with Open Access
Authors who publish with MedPulse International Journal of Radiology(Print ISSN: 2579-0927) (Online ISSN: 2636 - 4689) agree to the following terms: Authors retain copyright and grant the journal right of first publication with the work simultaneously licensed under a Creative Commons Attribution License that allows others to share the work with an acknowledgement of the work's authorship and initial publication in this journal. Authors are permitted and encouraged to post links to their work online (e.g., in institutional repositories or on their website) prior to and during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work. |
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.