 Home
Home
|
Table of Content Volume 16 Issue 1 - October 2020
Evaluation of soft tissue tumors by MRI in Telangana population
Rakesh Bayyavarapu1*, Lakshmi Sindhura Nadella2
1,2Assistant Professor, Department Of Radiology, Mediciti Institute Of Medical Sciences, Ghanpur, Medchal-501401. (Telagana), India. Email: bayyavarapurakesh@gmail.com
Abstract Background: MR Imaging has become established as an important cross sectional study to evaluate soft tissue tumors. Method: 85 patients having soft tissue were made to MRI examination 1.5 T Philips Achiva MRI scanner using a surface coil with size of location of lesion. Axial T1, T2, STIR, T2 sagittal and coronal STIR were performed. Results: 25 (29.4%) had lipoma, 12 (14.1%) Benign myofibroblastic proliferation, 10 (11.7%) Fibromastosis, 2 (2.35%) Lyphangioma, 3 (3.52%) glomus tumor of middle finger 11 (12.9%) nerve sheath tumor, 8 (9.41%) malignant fibrous histocytoma, 6 (7.05%) synovial sarcoma, 6 (7.05%) fibro sarcoma 2 (2.35%) had liposarcama, malignant tumor in lower limbs were 2 (2.35%) left LL, 4 (4.70%) right LL malignant fibrous histocytoma, 4 (4.70%) in life LL, 2 (2.3%) in right LL synovial sarcoma, 1 (1.17%) left LL, 4 (4.70%) in left LL fibro sarcoma, 1 (1.17%) in left LL, 2 (2.35%) in right LL was observed. Conclusion: This perspective study will be useful to evaluate role of MRI in characterizing the soft tissue tumors with histo-pathological findings so that further spreading of malignancy can be prevented and treat the patients efficiently. Key Words: Benign, Malignant, Sigma GE MRI, LL = Lower limb.
INTRODUCTION MRI images are currently considered superior to CT for imaging soft tissue tumors1,2 soft tissue sarcomas (STS) can arise almost anywhere in the body. Various types of STS include malignant fibrous histiocytoma, liposarcoma, synovial sarcoma, angiosarcoma, etc. Imaging is required to confirm the clinical diagnosis, to delineate the extent and for staging MRI provides superior soft tissue contrast, allows multi-planar image acquisition, obviates iodinated contrast agents and ionizing radiation and is divided of streak art crafts commonly encountered with CT3. Local staging is best accomplished using MRI, which can accurately depict the anatomic spaces and structures involved by tumor4. Hence to evaluate the soft tissue tumors of both extremities were visualised to know the staging of malignancies.
MATERIAL AND METHODS 85 patients aged between 8-70 years referred to Radiology department of Mediciti institute of Medical Sciences, Ghanpur, Medchal-501401. (Telannaga) were studied. Inclusion Criteria: Clinically suspected to have soft tissue tumors involving extremities were selected for study. Exclusion Criteria: The patients having venous Malformations hemiangiomas, intravenous malformations, soft tissue tumors not involving extremities. HIV positive patients were excluded for the study. Procedure: Every patients was made to be in supine position and MRI examination were done with 1.5 T Philips Achiva MRI scanner using a surface coil with size of the coil dependent on the size and location of the lesion. Axial T1, T2, STIR, T2 sagittal and coronal STIR are performed. For optimal sagital to noise ratio and spatial resolution, MR imaging examinations are performed with the smallest coil that fits tightly around the body part being studied while covering the entire lesion. Images are obtained 3- to 10 mm collimation; a 1- to 2-mm inter space gap to reduce cross – talk between consecutive section, one to two acquisitions; a 192 x 256 matrix (or 256 x 256 if more detail is desired) and the smallest field of view possible. Thinner slice (3 to 5 mm) is preferred for the evaluation of small lesions and through areas of maximum interest, where thicker slices (6 to 10 mm) are used for a general survey of larger lesion or entire extremity. The duration of study was September 2018 to July 2020. Statistical analysis: Types of benign and malignant tumors were segregated and classified with percentage. The analysis was done SPSS software. The ratio of male and females were 2:1.
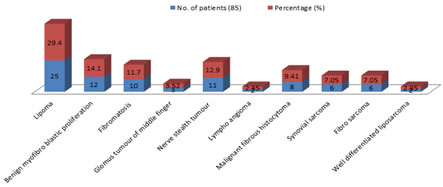
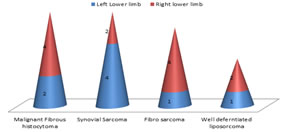
OBSERVATION AND RESULTS Table-1: Study of various to soft tissue tumors – 25 (29.4%) had lipoma, 12 (14.1%) had Benign myofibroblastic proliferation 10 (11.7%) had Fibromastosis 3 (3.52%) had glomus tumour of middle finger, 11 (12.9%) nerve sheath tumour. 2 (2.35%) had lympbangioma, 8 (9.41%) had malignant fibrous his cytoma, 6 (7.05%) synovial sarcoma, 6 (7.05%) fibro-sarcoma, 2 (2.35%) had well differentiated liposarcoma. Table-2: Study of malignant tumors in lower limb – 2 (2.35%) in left-lower limb, 4 (4.70%) right lower limb, (LL) of malignant fibrous histocytoma was observed, 4 (4.70%) synovial sarcoma in left LL and 2 (2.35%) in right LL. 1 (1.17%) of fibro sarcoma in left LL and 4 (4.70%) in right LL. 1 (1.17%) well differentiated liposarcoma in left LL, 2 (2.35%) in right LL.
Table 1: Study of various soft tissue tumors/ with percentage
Table 1: Study of various soft tissue tumours with percentage
Table 2: Study of Malignant tumors in lower limbs
Table 2: Study of Malignant tumours in lower limbs
DISCUSSION The present study of Evaluation of soft tumors by MRI in Telangana population, 25 (29.4%) lipoma, 12 (14.1%) benign myofibroblastic proliferation, 10 (11.7%) Fibromatosis, 3 (3.52%) glamus tumour of middle finger 11 (12.9%) nerve sheath tumor, 2 (2.35%) lymphangioma, 8 (9.41%, 6 (7.05%) synovial sarcoma, 6 (7.05%), 2 (2.35%) well differentiated liposarcoma (Table-1). Malignant tumors in lower limb, (LL) were 2 (2.35%) right LL, 4 (4.70%) had malignant fibrous histocytoma, 4 (4.70%) in left LL, 2 (2.35%) in right LL synovial sarcoma, 1 (1.17%) in left LL, 4 (4.70%) in right LL had fibrosarcoma, 1 (1.17%) in left LL, 2 (2.35%) in right LL had well differentiated liposarcoma (Table-2). These findings were more or less in agreement with previous studies 5,6,7. For any given mass regardless of cause, margins were typically better defined on T2 – Weighted image. Benign and malignant causes were not readily distinguished on the basis of margins 8. The over whelming majority of both benign and malignant lesions displayed intensity equal to less than that of skelet al. muscle on T1 weighted pulse sequences on the other hand malignant tumors including synovial sarcomas, soft tissue myxoid chondro sarcomas, neurofibrosarcoma, had signal intensity was T2 approximating that of sub-subcutaneous fat. Hence no unique features have been identified to reliably distinguish benign or malignant soft tissue lesions 9. It was also reported that, benign soft tissue lesions may appear on MRI as poorly defined but it remained controversial in many cases. But in the case of fatty tumours were found to be intramuscular lipomas in which the fatty elements predominated, although the tumor was inhomogeneous on MR because of inter spread regions of decreased signal on both pulse sequences. Hence benign fatty tumors are easily indentified on both CT and MR10. Sub acute hemorrhages’ were diagnosed easily because of high signal intensity on both T1 and T2 weighted pulse sequences.
SUMMARY AND CONCLUSION MR of benign fatty tumors, Pigmented villonodular synovitis, haemangioma and hematomas can be quite characteristic images, although not pathognomonic. There are no reliable criteria to distinguish the MR images of malignant from benign soft tissue tumors or tumor like masses. The MR images only reflect underlying lesion morphology like fat content, hemosiderin deposition, cyst formation, haemorrhage etc but not the specific histology. Hence histo-pathological reports can only confirm the diagnosis. This research work was approved by ethical committee of MediCii institute of medical sciences, Ghanpur Medchal – 501401. (Telangana)
REFERENCE
Policy for Articles with Open Access: Authors who publish with MedPulse International Journal of Radiology (Print ISSN: 2579-0927) (Online ISSN: 2636-4689) agree to the following terms: Authors retain copyright and grant the journal right of first publication with the work simultaneously licensed under a Creative Commons Attribution License that allows others to share the work with an acknowledgement of the work's authorship and initial publication in this journal. Authors are permitted and encouraged to post links to their work online (e.g., in institutional repositories or on their website) prior to and during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work.
Height, IVDL-Intervertebral Disc Length
Policy for Articles with Open Access
Authors who publish with MedPulse International Journal of Radiology(Print ISSN: 2579-0927) (Online ISSN: 2636 - 4689) agree to the following terms: Authors retain copyright and grant the journal right of first publication with the work simultaneously licensed under a Creative Commons Attribution License that allows others to share the work with an acknowledgement of the work's authorship and initial publication in this journal. Authors are permitted and encouraged to post links to their work online (e.g., in institutional repositories or on their website) prior to and during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work. |
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.